
Introduction to Communication in Nursing by Edited by Jennifer Lapum; Oona St-Amant; Michelle Hughes; and Joy Garmaise-Yee is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, except where otherwise noted.
Introduction to Communication in Nursing by Edited by Jennifer Lapum; Oona St-Amant; Michelle Hughes; and Joy Garmaise-Yee is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, except where otherwise noted.
1
Communication for the Nursing Professional – 1st Canadian Edition, 2020
This open access textbook is intended to guide best practices in communication in the context of the nursing profession. The resource addresses communication theory, therapeutic communication and interviewing, and interprofessional communication as it relates to nursing. This resource is designed for students in undergraduate nursing programs. The project is supported and funded by the Ryerson University Faculty of Community Services Publication Grant.
Level of Organization
Chapter 1 – Introduction to Communication and Communication Theory in Nursing
Chapter 2 – Therapeutic Communication and Interviewing in Nursing
Chapter 3 – Interprofessional Communication in Nursing
About the Authors
Jennifer Lapum, PhD, MN, BScN, RN, Professor, Daphne Cockwell School of Nursing, Ryerson University, Toronto, Ontario, Canada
Oona St-Amant, PhD, MScN, BScN, RN, Associate Professor, Daphne Cockwell School of Nursing, Ryerson University, Toronto, Ontario, Canada
Michelle Hughes, MEd, BScN, RN, Professor, School of Community and Health Studies, Centennial College, Toronto, Ontario, Canada
Joy Garmaise-Yee, DNP, MN, RN, CNE, Professor, Sally Horsfall Eaton School of Nursing, George Brown College, Toronto, Ontario, Canada
Charlotte Lee, PhD, BScN, RN, Assistant Professor, Daphne Cockwell School of Nursing, Ryerson University, Toronto, Ontario, Canada
Contact person
Dr. Jennifer L. Lapum
jlapum@ryerson.ca
415-979-5000 ex. 556316
@7024th patient
350 Victoria St., Toronto, ON, M5B 2K3
Ryerson University
Note to Educators Using this Resource
We encourage you to use this resource and would love to hear if you have integrated some or all of it into your curriculum. If you are using it in your course, please consider notifying Dr. Lapum and include the course/program and the number of students.
Acknowledgments
Meera Chawda, BScN student, Student Assistant, Ryerson University
Linn Clark, Editor, Toronto, Ontario, Canada
Frances Dimaranan, BScN student, Student Assistant, Ryerson University
Ann Ludbrook, Copyright and Scholarly Engagement Librarian, Ryerson University
Jeevan Marway, BScN, RN, MN Student, Artist and Infographic expert, Ryerson University
McKenzie Quevillon, BScN, RN, MN student, Multimedia Developer, Ryerson University
Nada Savicevic, MA Interactive Design, MArch, BScEng, Educational Developer, Centre for Excellence in Learning and Teaching, Ryerson University
Hilary Tang, BScN, RN, The Hospital for Sick Children, Front Cover Artist
Sally Wilson, Web Services Librarian, Ryerson University
Customization
This textbook is licensed under a Creative Commons Attribution 4.0 International (CC-BY NC) license except where otherwise noted, which means that you are free to:
SHARE – copy and redistribute the material in any medium or format
ADAPT – remix, transform, and build upon the material for any purpose, even commercially.
The licensor cannot revoke these freedoms as long as you follow the license terms.
UNDER THE FOLLOWING TERMS:
Attribution: You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
No additional restrictions: You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
Notice: You do not have to comply with the license for elements of the material in the public domain or where your use is permitted by an applicable exception or limitation.
No warranties are given. The license may not give you all of the permissions necessary for your intended use. For example, other rights such as publicity, privacy, or moral rights may limit how you use the material.
Content that is not taken from the OERs noted below or copyrighted material should include the following attribution statement:
© 2020 Ryerson University. Licensed under a Creative Commons Attribution 4.0 International License (CC-BY NC). Communication for the Nursing Professional (1st Canadian edition) by Jennifer L. Lapum, Oona St-Amant, Michelle Hughes, Joy Garmaise. Download this book for free at: https://pressbooks.library.ryerson.ca/communicationnursing/
Attribution statement
Part of the content of this textbook contains material from two Open Educational Resources (OERs). The OERs adapted include:
The Complete Subjective Health Assessment by Jennifer L. Lapum, Oona St-Amant, Michelle Hughes, Paul Petrie, Sherry Morrell, and Sita Mistry is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
For information about what was used and/or changed in this adaptation, refer to the statement at the bottom of each page where applicable.
I
By Jennifer L. Lapum, Oona St-Amant, Michelle Hughes, and Joy Garmaise-Yee
1
By the end of this chapter, you will:
2
When you think of communication, talking to another person or texting them might come to mind first. However, while talking and texting are methods of communication delivery, they are not representative of a comprehensive definition of communication.
A more comprehensive understanding of communication refers to the sharing of information, ideas, and feelings, typically aimed at mutual understanding. In this way, you must consider the sender, the recipient, and the transaction. Simply put, the sender is the person sharing the message, the recipient is the person receiving and interpreting the message, and the transaction is the way that the message is delivered and the factors that influence the context and environment of the communication. As you can see, communication is a complex process. It involves more than just what you say and takes many forms as reflected in Figure 1.1.

Figure 1.1: Forms of communication.
There are three types of communication:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=80#h5p-1



3
Professional communication is an important part of becoming a nurse and being a nursing student. You are entering a “profession” which means there are certain expectations in terms of your professional conduct specifically in terms of how you communicate.
Professional communication involves a level of formality and is an important component of your post-secondary nursing education. It is different than the informal communication that you may engage in with your friends and family. It also applies to your verbal and written communication including emails.
The principles of professional communication include being truthful, accurate, clear, and both concise and comprehensive. For example, you should say or write something in a succinct and short way while also including all relevant information. You should also have a professional tone that is conveyed through appropriate greetings, complete sentences, and grammar. In order to be professional, you need to know your audience; both the content and form of your message should be tailored to your audience.
Here are some tips to follow in terms of professional communication:
Because a lot of communication occurs electronically, it is important to consider how to construct an email. Here are some tips:
Points of Consideration
Addressing and referring to your instructor
Students are often uncertain how to address their instructors. It is okay to ask your instructors how they would like to be addressed. Until you know how, you should refer to them as “Professor X” (insert their surname) or “Dr. X” (insert their surname).
Although some instructors may invite you to use their first name, it is part of professional communication etiquette to use “Professor X” or “Dr. X” (including both their first and last name) when referring to them to others. In addition to ensuring professional communication, this helps to provide clarity if your instructors share a first or last name with another instructor.
Example: Dr. Huang is your course instructor, and they have encouraged you to reach out to another professor to discuss potential research opportunities. Although Dr. Huang has given you permission to call her Lisa in the classroom, you should always refer to them as Dr. Lisa Huang in communication with others. Thus, when initiating communication with the instructor that Dr. Huang has referred you to, you may consider a beginning such as: “Dear Dr. Hameed. I am a student in the undergraduate year one nursing communication course with Dr. Lisa Huang. Dr. Huang has encouraged me to reach out to you about potential research opportunities because of my interest in critical feminism.”
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=82#h5p-4
4
Conflict is a variance in perceptions and opinions that involves a perceived or actual threat.
It is important to avoid thinking of threat as an intention to inflict physical harm or pain upon someone. Rather, consider threat as an unfavourable situation and force that may adversely affect you.
Threat is embedded in conflict because a person’s perception or position quickly becomes part of who they are (i.e., their self concept) and as such, an opposition to this perception is considered “a threat to self” (De Dreu & van Knippenberg, 2005, p. 345). A perceived threat or an actual threat happens with conflict because you perceive that something/someone is challenging your beliefs or needs and may affect your sense of self or the relationship you have with them.
Have you ever perceived a threat when having a difference of opinion or disagreed with someone else? Have you felt a sense of threat in a setting where there are deeply engrained power dynamics? Have you been engaged in a class discussion where you had a different way of seeing things than another person? Have you had a concern about a university/school’s policy? Have you received a grade on a paper from a professor and you did not agree with it? You may feel worried to speak up about an issue because the other person has a different perspective than you. You may fear that if you speak up, they will think you are ignorant or that it may affect your relationship with them.
These are all examples of conflict, and are associated with a perceived threat or actual threat.
Conflict can trigger strong emotions and has the potential to negatively affect how you respond and how you communicate.
Consider how you have responded to conflict in the past. Did you ignore or avoid the conflict? Did you take the disagreement personally? Did you engage in intense and relentless argument? Have you ever not addressed it with the person, but instead posted on social media or gossiped to a friend or peer? These are all ineffective ways to deal with conflict because it never resolves the problem – the conflict.
It is important to understand and address conflict as it is a part of any relationship including those in the educational and professional settings. There is the possibility that you can transform how you perceive conflict, and thus, how you address conflict – this is the positive lens of conflict.
Points of Consideration
The positive lens of conflict
A starting point is to transform how you view conflict. Have you ever considered viewing conflict from a positive lens? Conflict suggests that you have an opinion that you hold as meaningful or important. In itself, this is a good thing. It can be beneficial to approach conflict as an opportunity. You can learn and grow by truly listening to another person’s view and sharing your own. Part of this is seeking to understand what the perceived threat is for you and for the other person(s). If approached professionally, this sharing can help you feel good that you have shared your opinion, why it matters to you, and participated collaboratively and respectfully to manage the conflict. Additionally, by learning and growing while engaging professionally with another person, this can sometimes create a connection that cultivates your relationship with them. It can also add to a positive resolution related to the conflict with the potential for creative and divergent thinking.
References
De Dreu, C., & van Knippenberg, D. (2005). The possessive self as a barrier to conflict resolution: Effects of mere ownership, process accountability, and self-concept clarity on competitive cognitions and behavior. Journal of Personality and Social Psychology, 89(3), 345-357. https://doi.org/10.1037/0022-3514.89.3.345
5
Conflict resolution is about finding a reasonable solution to varying perspectives. This may involve you and the other person(s) sharing your perspective to enhance understanding of the issue. It may result in you or the other person shifting your perspective in a way that a reasonable solution is arrived upon related to the conflict. Often, when conversation goes beyond the disagreement on the surface and instead explores the perceived or actual threat on each side, more options for compromise and resolving the conflict emerge.
Professionalism should always guide how you approach and manage conflict. In educational institutions and in nursing, professionalism is essential. As a student, specifically a nursing student, you are developing your professional self as a nurse. This means that you have a responsibility to uphold values of honesty, respect, and integrity in all your interactions.
Engaging in effective conflict resolution takes practice. Remember, as nursing student, you are learning and growing in so many ways. As such, engaging in reflection on how you participate in conflict resolution in terms of what was effective and what was not effective is important to your professional development.
Fortunately, conflict resolution is a skill that you can learn, and that is a good thing. There are several conflict resolution strategies that can inform your communication:
Points of Consideration
Courage and conflict
Addressing conflict sometimes takes courage. You may feel uncertain about how to address it and frightened that it will affect your relationship with the other person(s). There may be power dynamics involved. For example, you may need to address an issue with a person in a position of authority, such as a class professor or clinical instructor. Be courageous and act despite the fear, vulnerability, and uncertainty you may feel. It is better to be direct with the person you have a conflict with than to harbour resentment. Recognize this fear, vulnerability, and uncertainty. But also recognize the positive feelings associated with being courageous. You accomplish something important when you deal with conflict. You get courageous by being courageous.
One strategy to help you address the conflict is to write it down on a piece of paper and say it out loud. This can help you identify and acknowledge emotions attached to the conflict. Then when you address the conflict with the individual, you can focus on the issue and not the personal emotions which could impact the discussion. Ask to meet with the person and have a face-to-face discussion as opposed to trying to talk about the issue via email or text.
Case Example
Consider a situation in which a family is upset about the nursing care their loved one is receiving, and tells you that after watching you do an assessment on the client, you “clearly don’t know what you’re doing.”
Analysis
The family member’s words could cause a sense of threat for you. Perhaps you may fear a sense of being falsely accused and reported and are unsure of the consequences that might ensue. You may get very defensive and insist that you did “nothing wrong.” On the other hand, this family may be feeling a very different threat, i.e., perhaps they fear their loved one’s condition is deteriorating, and they may lose them soon. Any small error (or perceived error) in their loved one’s care may trigger fear around losing them. Having a conversation with the family to acknowledge the threat (i.e., fear) they are experiencing may be beneficial to resolving the conflict over their perception of your care.
6
Many people use social media (e.g., TikTok, Instagram, Twitter, Facebook, WhatsApp) as a way to share and engage with others and as a form of education and entertainment. However, as a nursing student, you are legally obligated to uphold a Code of Conduct in both personal and professional social media posts.
A Code of Conduct is a standard of practice that sets expectations and outlines norms and responsibilities of a professional. It establishes and formalizes common values within the profession and is intended to govern behaviour. The College of Nurses of Ontario (CNO, 2019a) has articulated a Code of Conduct with six guiding principles:
As a nursing student, you are expected to uphold the same practice standards as a Registered Nurse.
With the advent of social media, as a Registered Nurse and a nursing student you are expected to uphold the Code of Conduct now more than ever. Even though you may use social media in your personal life, you are still expected to maintain professionalism. For example, under the Code of Conduct, nurses and nursing students are expected to treat their colleagues with respect on social media. Nurses and nursing students who use social media are not allowed to share patient information or post confidential information, even on private accounts.
The CNO (2019b) Practice Standards documents states “nurses have a duty to uphold the standards of the profession, conduct themselves in a manner that reflects well on the profession, and to participate in and promote the growth of the profession” (p. 11). As such, there is a collective responsibility to contribute to the positive image of the nurse, and actively promote the reputation of a nurse. Posting information on social media that is unethical, unlawful, and disgraces a colleague in your practice or educational institution or dishonours the image of the nurse could result in serious consequences to licensure.
Case Example
In 2015, a Registered Nurse from Saskatchewan took to social media to air her grievances about the quality of care her grandfather received in long-term care. In her Facebook posting, she named the institution that cared for her grandfather and urged the institution do better in future patient care. In her posting, she did not explicitly name any healthcare providers, nor did she use inflammatory language, but she referred to her grandfather’s care as “sub-par”. In 2016, she was found guilty of professional misconduct by the Saskatchewan Registered Nurses Association (SRNA) and was ordered to pay a $1,000 fine and $25,000 towards costs for the tribunal. In 2020, Saskatchewan’s highest court overruled the disciplinary decision and fine.
Analysis
The nurse in this case was originally found guilty of misconduct for harming the reputation of nurses by going to social media to make complaints. It was also noted that other formal complaint channels (such as managers of the institution), would have been a more appropriate alternative to make change. Furthermore, the legal team for the SRNA argued that all facts should have been collected before making allegations against the institution. Ultimately, the decision was overturned, however this case emphasizes the importance of being intentional, deliberate, and professional when engaging on social media.
Your employer or educational institution may or may not have specific policies related to the use of social media outside of the workplace. It is important as an employee or a student to be aware of any institutional guidelines for social media use. Furthermore, the CNO will consider situations of misconduct as a regulatory body.
Examples of violations on social media:
Points of Consideration
24-hour Rule
Part of the lure of social media is the immediacy with which you share information or receive feedback. Social media has also become a common place to air grievances or share complaints. You can rally support or oppose views with the click of button. However, given that a social media post can have serious repercussions on your career as a nurse and a student, it is important to give additional consideration to what you post online. One strategy to assist is the 24-hour rule, which means when you are uncertain of the effects of your post or you sense that your words may be provocative, wait 24hours and think through your decision. It does not hurt to seek feedback from trusted peers as well.
Additionally, if you have a grievance or a complaint, it is best to address it directly with the person or institution involved. Recall how to address conflict through a positive lens.
7
Communication is a complex process, and it is sometimes difficult to determine where or with whom a communication encounter starts and ends. Models of communication simplify the process by providing a visual representation of the various aspects of a communication encounter. Some models explain communication in more detail than others, but even the most complex model cannot recreate what we experience in any given moment of a communication encounter.
Models still serve a valuable purpose because they define communication and allow you to see specific concepts and steps within the process of communication. Models give rise to ideas or nuances that you may not have considered. When you become aware of how communication functions, you can think through your communication encounters more deliberately, which can help you better prepare for future communication and learn from your previous communication.
The three models of communication discussed in this chapter are:
Although these models of communication differ, they contain some common elements. The first two models, the Transmission Model and the Interaction Model, include the following parts: participants, messages, encoding, decoding, and channels. In communication models, participants are the senders and/or receivers of messages in a communication encounter. The message is the verbal and nonverbal content being conveyed from sender to receiver. For example, when you say “Hello!” to your friend, you are sending a message of greeting that will be received by your friend.
The internal cognitive process that allows participants to send, receive, and understand messages includes the processes of encoding and decoding.
Of course, you don’t just communicate verbally – you have various options, or channels, for communication. Encoded messages are sent through a channel, or a sensory route on which a message travels, to the receiver for decoding. While communication can be sent and received using any sensory route (sight, smell, touch, taste, or sound), most communication occurs through visual (sight) and/or auditory (sound) channels. If your roommate has headphones on and is engrossed in a video game, you may need to get their attention by waving your hands before you can ask them about ordering Thai food.
Now, let’s examine the three models of communication discussed in this chapter: Transmission, Interaction, and Transaction Models.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=84#h5p-5
With editorial changes, adapted from:
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
8
The Transmission Model of communication (see Figure 1.2) describes communication as a linear, one-way process in which a sender intentionally transmits a message to a receiver (Ellis & McClintock, 1990). This model focuses on the sender and the message within a communication encounter. Although the receiver is included in the model, this role is viewed as more of a target or end point rather than part of an ongoing process. In this case, one presumes that the receiver either successfully receives and understands the message or does not. As such, this model is not representative of effective communication for how messages are received.
![]()
Figure 1.2: The Transmission Model of Communication
Because this model is sender- and message-focused, responsibility is put on the sender to help ensure the message is successfully conveyed. This model emphasizes clarity and effectiveness, but it also acknowledges that there are barriers to effectively sending communication. Noise is anything that interferes with a message being sent between participants in a communication encounter. Even if a speaker sends a clear message, noise may interfere with a message being accurately received and decoded. The Transmission Model of communication accounts for environmental and semantic noise.
A client is seeking care for a suspected urinary tract infection. A nurse communicates to a client that they need to provide a urine sample and fully empty their bladder. The nurse speaks quietly in an attempt to maintain confidentiality because the client is sitting near a waiting room full of people. The client provides a urine sample but does not follow the proper technique for collecting the sample.
Analysis: In this case, the message was successfully sent to the client as evidenced by the client’s action and response to the request. The interference of environmental noise (nurse speaking softly) and semantic noise (nurse not providing complete instructions) affected how the message was decoded and ultimately the accuracy of the urine sample results.
Pros: This model spotlights the sender and the possible noise that can affect the transmission of communication.
Cons: This model is limited because it privileges how the sender communicates, with little attention paid to how the message is received. It is also limited in terms of the message, because it simply evaluates whether or not the message was delivered. The example above illuminates how detail and nuance should be attended to when communicating.
In Figure 1.3, click on any features that represent environmental noise.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=86#h5p-32
Figure 1.3: Elements of environmental noise.
With the exception of the nursing example, content was adapted from (with editorial changes):
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
9
The Interaction Model of communication (see Figure 1.4) describes communication as a process in which participants alternate positions as sender and receiver and generate meaning by sending messages and receiving feedback within physical and psychological contexts (Schramm, 1997). Rather than illustrating communication as a linear, one-way process, this model incorporates feedback, which makes communication a more interactive, two-way process.
Feedback includes messages sent in response to other messages. For example, a patient may ask you a question in response to health information you provide them. The inclusion of a feedback loop allows a more complex understanding of the roles of participants in a communication encounter. Rather than having one sender, one message, and one receiver, this model has two sender-receivers who exchange messages. Each participant alternates roles as sender and receiver in order to keep a communication encounter going. You alternate between the roles of sender and receiver very quickly and often without conscious thought.
The Interaction Model of communication is more interaction-focused. In this model, communication isn’t judged as effective or ineffective based on whether or not a single message was successfully transmitted and received. In fact, this model acknowledges that because so many messages may be sent at one time, many of them may not even be received. Some messages are also unintentionally sent. Thus, the model acknowledges that communication is nuanced and complex.
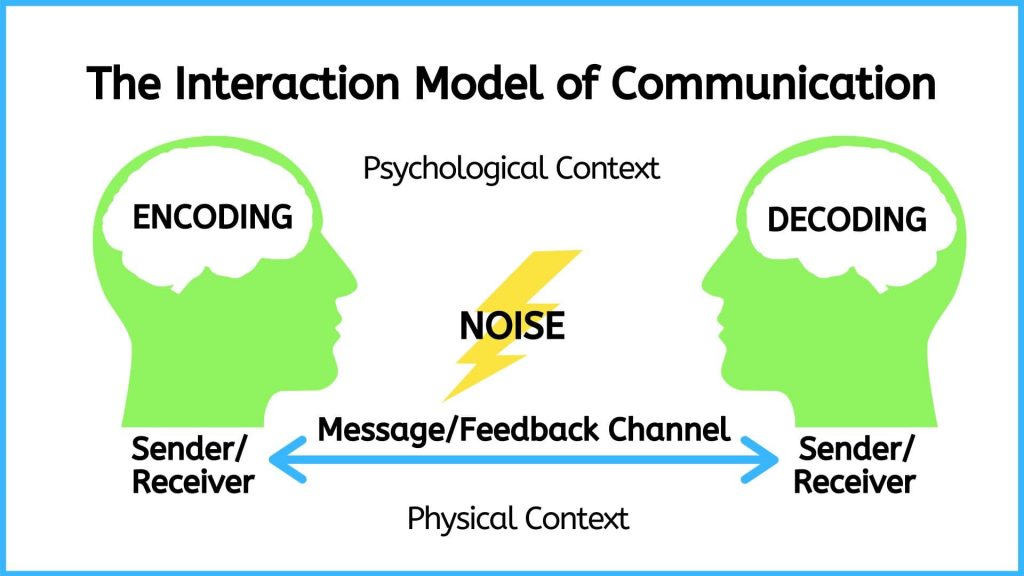
Figure 1.4: The Interaction Model of Communication
The Interaction Model takes physical and psychological context into account.
A nurse has worked 11 hours and is attending to a client recently admitted to the hospital. The 68-year-old client is waiting for a bed and is stationed on a stretcher in the emergency room hallway. The client sought emergency care after experiencing severe abdominal pain and passing substantial blood when having a bowel movement. The client was informed that it is likely they have end-stage bowel cancer but is still awaiting a formal diagnosis and referral to oncology (cancer specialist). The nurse asks the client if the nurse can take a set of vital signs. The client responds “yes.” The nurse also tries to make the client comfortable by adjusting the head of the stretcher and asks the client if they need anything. The client has many questions and concerns and has not had anything to eat or drink in several hours but responds “no.” The nurse says “OK, well let me know if you need anything.”
Analysis: The physical context that played an important role in this example is the lack of privacy and overstimulation in a waiting area located in an emergency room hallway. The physical space likely played a role in the client’s response, which resulted in the client’s needs being unmet. The psychological context relates to the burden of a looming terminal diagnosis juxtaposed with the undignified environment. The nurse may have sensed that probing further about the client’s needs and current state of mind was needed but may have been physically tired and emotionally drained after working 11 hours. All these factors contributed to the interaction between the nurse and the client.
Pros: This model allows the user to reflect on the environment (both physical and psychological) and how this contributes to good communication. In this case, communication was deemed inadequate because the interaction was limited by the environmental context.
Cons: Although this model attends to the broader context in which communication takes place, it is also inattentive to social, political, and economic realities that shape communication. In other words, it does not consider how the nurse’s and the client’s identity inform their communication with each other.
Remixed with original content and adapted, with editorial changes, from:
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
10
The Transaction Model of communication (see Figure 1.5) differs from the Transmission and Interaction Models in important ways, including the conceptualization of communication, the role of sender and receiver, and the role of context (Barnlund, 1970).
The Transaction Model of communication describes communication as a process in which communicators generate social realities within social, relational, and cultural contexts. In this model, nurses don’t just communicate to exchange messages; they communicate to:
In short, you don’t communicate about your realities; communication helps to construct your realities.
The roles of sender and receiver in the Transaction Model of communication differ significantly from those in the other models. Instead of labeling participants as senders and receivers, the people in a communication encounter are referred to as communicators. Unlike the Interaction Model, which suggests that participants alternate positions as sender and receiver, the Transaction Model suggests that you are simultaneously a sender and receiver.
For example, when you first meet a client, you send verbal messages saying hello, who you are, and why you are there. Before you are done your introduction, the client is reacting nonverbally. You don’t wait until you are done sending your verbal message to start receiving and decoding the nonverbal messages of the client. Instead, you are simultaneously sending your verbal message and receiving the client’s nonverbal messages. This is an important component of this model because it helps you understand how you can adapt your communication. For example, in the middle of sending a verbal message, you can adapt your communication in response to the non-verbal message you are simultaneously receiving from your communication partner.
![]()
Figure 1.5: The Transaction Model of Communication
The Transaction Model also includes a more complete understanding of context. The Interaction Model portrays context as physical and psychological influences that enhance or impede communication. While these influences are important, the model focuses on message transmission and reception. Because the Transaction Model of communication frames communication as a force that shapes your realities before and after specific interactions occur, it must account for contextual influences outside of a single interaction. To do this, the Transaction Model considers how social, relational, and cultural contexts frame and influence communication encounters.
Here is a short description of each context:
You need skills to adapt to shifting contexts, and the best way to develop these skills is through practise and reflection.
A 42-year-old client and her partner are attending a fertility clinic awaiting intrauterine insemination with donor sperm. It is the client’s third attempt at the procedure, and she is becoming concerned that she may never get pregnant. The stress of getting pregnant has weighed on the client and her partner. They got into an argument on the way to clinic and are not speaking to each other. Both the client and her partner are South Asian and have experienced both racial and sexual discrimination in their past encounters with the healthcare system. A 59-year-old nurse of European decent enters the room and both the client and her partner are on their phones and barely look up at the nurse. The nurse is polite and completes her care plan. The nurse interprets their lack of attention as indifference to the situation and does not bother to counsel the client and her partner further, assuming it is not necessary. The nurse also assumes they have no questions, because it is their third attempt at the procedure.
Analysis: This example sheds light on the sort of nuances involved when communicating with clients. In this case, the nurse reads the lack of eye contact and engagement as a social convention that relays disinterest. From a relational standpoint, the nurse was unfamiliar with the couple and relied on a brief encounter, combined with information from the client’s chart. From a cultural standpoint, a shared understanding and space is needed to engage in discussions affected by culture. In this case, because of the social and relational misalignment, it was not likely the nurse and client/partner would engage in meanings of culture and socio-political context in relation to their care.
Pros: This approach offers more breadth and understanding of how intra-personal, inter-personal, and contextual factors are at play in communication. People often make assumptions predicated on these contextual factors, and therefore it is important to acknowledge these elements in practising and learning about good communication.
Cons: This approach requires analysis and critical reflection. It requires a broader understanding of historical, political, and social structures that affect communication. The specific factors affecting a particular communication encounter may or may not be possible to uncover.
Remixed with original content and adapted, with editorial changes, from:
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
11
See Table 1.1 for a summary of the Transmission, Interaction, and Transaction Models of communication.
Table 1.1: Communication Models
Models | Foci |
Transmission Model | Frames communication as a thing, like an information packet, that is sent from one place to another. From this perspective, communication is defined as sending and receiving messages. |
Interaction Model | Frames communication as an interaction in which a message is sent and then followed by a reaction (feedback), which is then followed by another reaction, and so on. From this perspective, communication is defined as producing conversations and interactions within physical and psychological contexts. |
Transaction Model | Frames communication as integrated into social realities in such a way that it helps communicators not only to understand them, but also to create and change them. |
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=92#h5p-8
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=92#h5p-9
12
Most people are born with the capacity and ability to communicate, but everyone communicates differently. This is because communication is learned rather than innate. As you have already seen, communication patterns are relative to context and culture.
As discussed earlier, context is a dynamic component of the communication process. Culture and context also influence how you perceive and define communication. Western culture tends to place more value on senders than on receivers, and on the content rather than the context of a message, like the Transmission Model. These cultural values are reflected in our definitions and models of communication. Western culture also influences communication within the healthcare domain. However, you may not have been socialized within a Westernized culture, and you may not be caring for someone who was socialized within a Westernized culture. Therefore, it is important to reflexively examine how your own culture, beliefs, and norms influence your communication, and to be aware of how you communicate.
A key principle of communication is that it is symbolic. This means that the words making up language systems do not directly correspond to something in reality. Instead, words stand in for or telegraph something. The fact that communication varies so much among people, contexts, and cultures illustrates the principle that meaning is not exclusively inherent in the selection of words. For example, let’s say you go to France on vacation and see the word poisson on the menu. Unless you know how to read French, you will not know that the symbol (word) is the same as the English symbol fish. Those two words don’t look the same at all, yet they symbolize the same object. If you went by how the word looks alone, you might think that the French word for fish is more like the English word poison and avoid choosing that for your dinner. Putting a picture of a fish on a menu would definitely help a foreign tourist understand what they are ordering, because the picture is an actual representation of the object rather than a symbol for it.
All symbolic communication is learned, negotiated, and dynamic. You know that the letters b-o-o-k refer to a bound object with multiple written pages. You also know that the letters t-r-u-c-k refer to a vehicle with a bed in the back for hauling things. But if you learned in school that the letters t-r-u-c-k referred to a bound object with written pages and b-o-o-k referred to a vehicle with a bed in the back, that would make just as much sense, because the letters don’t actually refer to the object – the word itself only has the meaning that is assigned to it.
Everyone is socialized into different languages, but we also speak differently based on the situation we are in. For example, in some cultures it is considered inappropriate to talk about family or health issues in public. However, in other cultures, it wouldn’t be considered odd to overhear people in a hospital waiting room talking about their loved ones who are currently in surgery. Additionally, some communication patterns are shared by very large numbers of people and some are particular to groups – nurses, for example, who have their own terminology and expressions that might not make sense to others. These examples aren’t on the same scale as differing languages, but they still illustrate how communication is learned, and how rules and norms influence how we communicate.
Remixed with original content and adapted, with editorial changes, from:
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
13
In addition to models of communication, many theoretical approaches can be used to inform your communication with clients and families. The theoretical approach you select may depend on the client population you work with, the institution you work in, and personal preference based on your expertise and experience.
Common approaches that align with nursing and therapeutic communication are a trauma-informed approach, a relational inquiry approach, and an anti-racist approach. The following sections provide an overview of each approach with an accompanying case study as an example.
14
It is important for nurses to engage in communication from a trauma-informed approach, which involves integrating an understanding of the need for:
(Trauma-Informed Practice Guide, 2013, p. 12).
A trauma-informed approach can be used as one part of therapeutic communication. It involves emphasizing confidentiality, identifying the interview purpose, letting the client set the pace of the interview and shaping it based on their needs, and engaging in collaborative intervention so that the client is in control and empowered. As you apply this approach, you should always be thinking about how you can promote safety, control, and choice for the client.
Given how pervasive trauma is in clinical practice, a trauma-informed approach makes sense to incorporate into your communication and way-of-being with clients. This kind of approach is especially useful because you will often not know who has experienced trauma or the circumstances of their trauma. Trauma includes the emotional consequences of a distressing event (Centre for Addiction and Mental Health [CAMH], n.d.). Many circumstances can lead to trauma, including child abuse and neglect, sexual assault and intimate personal violence, bullying and harassment, as well as events such as car accidents, a death of someone close to you, natural disaster, and war.
Points of Consideration
Indigenous populations
Among Indigenous populations, historical and intergenerational trauma caused by Canada’s oppressive colonial policies and practices as well as the destructive effects of residential school systems takes the form of unresolved grief and trauma passed from one generation to the next (O’Neil et al., 2016; Mash et al., 2015). It has also led to a silencing of experiences (O’Neil et al., 2016), impacts on Indigenous identity (Lavallee & Poole, 2010), and has caused feelings of worthlessness, self-hatred, fear, and powerlessness (Chrisjohn & Young, 2006; Health Council of Canada, 2012), as well as mental health issues including anxiety, depression, post-traumatic stress disorder, and substance use and addictions (Assembly of First Nations, 1994; Brave Heart, 2003; Chrisjohn & Young, 2006; Mash et al., 2015; O’Neil et al., 2016).
Because the trauma-informed communication approach assumes the presence of trauma, it does not require the client to disclose their experience and thereby risk re-traumatizing them through repeated disclosure (Trauma-Informed Practice Guide, 2013).
See Case Study 1 for an example of a trauma-informed approach to interviewing.
A 19-year-old client presents alone at urgent care. The reason for seeking care noted on the client’s chart is: pain, swelling, and bruising on index and middle digits of the left hand, suspected fracture. Upon entry into the examination room, the nurse observes healed bruising under the client’s right eye and contusions on the client’s neck.
RN: Hello Franco Alonso, my name is Pita Kora, I will be your registered nurse today. You can call me Pita and my pronouns are she/her. What would you like me to call you and what pronouns do you use?
Client: Franco and he/him is fine.
Rationale: Introduce self using first and last name and explains designation – this action promotes accountability for your actions, as it demonstrates that you are taking responsibility through disclosure. Asking what the client would like to be called and their pronouns contributes to the client’s sense of control and wellbeing. It also conveys respect for their chosen identity.
RN: Everything we talk about will remain confidential and will only be discussed among healthcare team members involved in your care.
Rationale: This emphasizes confidentiality, including the parameters of who will be privy to the information. This is important to disclose and does not mislead the client to believe that any information they provide will end with you. Indeed, as a nurse you are required to report the data you collect. This honesty is especially important in a trauma-informed approach to build trust and ensure safety.
Client: Ok
Rationale: In this case, you wait for the client to acknowledge your statements, which conveys respect.
RN: Today I will ask you some questions related to your injury and then I will conduct a physical assessment. I will explain all steps as I go along. It will take about 15 or 20 minutes. Does that work for you?
Client: I think so…
Rationale: By proving the client with the purpose and general plan of the interview, you share control and minimize unpredictability. By asking the client if it works for them, you include them in the process and convey collaboration. Certainty and control are important parts of creating a safe space for dialogue.
RN: Can you tell me about what happened to your fingers, Franco?
Client: They were crushed in a car door. It really hurts. I think it may be broken.
Rationale: In this case, you ask an open-ended question without assumptions. This approach is better to begin with than a series of closed-ended questions directed by you. In this case, it is important to allow the client to share their story in their own words.
RN: Ok. I’m sorry to hear. That sounds painful. We will assess for any fractures. How long ago did this happen?
Rationale: You express empathy by responding to what the client said, instead of how the fingers look. It is important to respond to what the client is telling you to build trust. Also, the statement “we will assess for any fractures” offers the client reassurance that the injury will be attended and also acknowledges the initial concern that “it may be broken.” It is important to acknowledge the client’s concern and not dismiss their concern.
Client: Last week. I didn’t think much of it at first, but the swelling hasn’t gone away and the bruising seems to be getting worse. I wasn’t sure if I should come.
RN: Ok, sure, I can understand that. I noticed some other bruises under your right eye and on your neck. Are they related to your finger injury?
Rationale: You convey empathy by stating that you can understand the client’s choices/decisions without judgement. You ask a closed-ended question about other injuries but should allow the client to respond at their pace.
Client: Not really. I mean it happened around the same time but they aren’t related.
RN: Ok [allow for silent pause].
Rationale: Silence can be a powerful form of communication. It works in two ways in a trauma-informed approach: first, it conveys to the client that you are unhurried and invested in what they are saying; second, it can give the client an opportunity to think through their responses, which can alleviate pressure on the client and promote their self-determination.
Client: It’s kind of a long story. I’m sure you’re busy.
RN: I’ll make time. Tell me more.
Rationale: The client may be testing your interest and investment to gauge the level of trust. It is important to foster trust within the client and let them know you are reliable. If this isn’t possible at that moment, explain to the client why you may not have the time but when you will have the time. For example, “I have an urgent matter down the hall, but I will return in 5 minutes to discuss further.” In such cases, it is important to follow up on your promise and not let the client down, because this is likely to damage any trust built.
A trauma-informed approach creates a safe space for clients to engage in conversation and fosters control and choice. It does not require the client to disclose trauma. However, it creates a space in which the client may feel safe to speak about trauma, if relevant, at their own pace.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=98#h5p-10
15
Relational inquiry is defined as “the complex interplay of human life, the world, and nursing practice” (Doane & Varcoe, 2015, p. 3). This means that nurses must avoid looking at the client on a merely individual level (Doane & Varcoe, 2015). As per Doane and Varcoe, drawing upon relational inquiry involves the following elements of communication:
Relational inquiry is a kind of lens you can use to perceive the world. In contrast to an individualist approach, which privileges the individual as accountable for their actions and behaviours, relational inquiry brings into focus the internal dialogue of the client, their social system, and the broader context that influences their actions and your actions as a nurse (Doane & Varcoe, 2015). This approach to therapeutic communication is important because it can help you understand the client’s situation more fully, focus on what is important to them, and collaboratively work with the client to integrate this knowledge into the care.
See Case Study 2 for an example of a relational inquiry approach to interviewing.
An 8-year-old client, who uses the pronouns he/him, attends a pre-operative day surgery unit for tonsillectomy (tonsil removal) with a parent present. The client has a history of 6 strep throat infections with antibiotic treatment in the last 18 months. The client has no previous history of surgery or anaesthesia.
RN: Hello Peter Lin, my name is Ahsan Khan, I am a registered nurse. I will be caring for you until you go into surgery and then a surgical nurse will take over your care. You can call me Ahsan. What name would you like me to call you?
Client: Peter.
Rationale: You introduce yourself using first and last name and explain designation – this action promotes accountability. You explain the extent of the care being provided, including when it will end and who will take over care for the client at different stages of their procedure. This includes the client in the care plan and minimizes uncertainty about care provision.
RN: Okay, Peter. The information you share with me will only be shared with the healthcare team involved in caring for you. Before we begin, who is with you today?
Client: It’s my mom.
Rationale: You explain confidentiality at a developmentally appropriate level for an 8-year-old. Asking the client “who is with you today” allows the client to identify their relationship to their caregiver in their own words.
RN: [directed to mother] Hello, what would you me to call you?
Client’s mother: Please call me Wei.
Rationale: This approach includes the mother in the care and acknowledges her participation. Some providers refer to the parent as mom or dad as this reinforces the client (child) as the recipient of care and is also convenient for the provider for easy reference. However, calling the parent by their preferred name builds trust and rapport, acknowledges their humanity, and identifies them in the care process.
RN: Okay, Wei. [directed to both client and client’s mother] I will collect some information from you and then do a physical exam. It should take about 10 minutes. I can see in your chart here that you are scheduled for a tonsil removal and that you have signed a consent form. Can I answer any questions you have before we proceed?
Rationale: Repeating the preferred name of the client’s mother helps you remember the name, while also acknowledging the mother’s request. You offer the client and mother a timeline and plan to help them anticipate events. You invite any questions before conducting the subjective data collection. This can be a helpful tool for you to gauge the client and can also alleviate concerns up front.
Client and Client’s mother: Not really.
RN: Ok. Can you tell me about how you are feeling today, Peter?
Rationale: This question invites an intrapersonal response as it attends to feelings and emotions for the client. Most importantly, it acknowledges the importance of his thoughts and emotions as part of their care (rather than ignoring them) and gives you the opportunity to respond to any concerns.
Client: A little nervous. Will I be able to feel anything during surgery?
RN: No, you won’t feel anything during surgery. We will give you some medicine to put you into a deep sleep and when you wake up it will be over. We will also be giving you some medication for pain.
Rationale: Your response attends to the client’s concern directly by providing a definitive answer. In this case, you also anticipate the client’s concern for pain as the concept may not be well understood, given the developmental stage.
RN: How are you feeling, Wei?
Client’s mother: I’m little nervous to give Peter pain medications.
Rationale: The question invites the mother to share intrapersonal concerns about the client’s surgery. This conveys to the mother a family-centred approach, whereby they are also a care recipient.
RN: Tell me more about your concern.
Client’s mother: Well, you read so much nowadays about opioids and addiction problems caused by prescribed medications. I’m worried about Peter.
Rationale: This approach invites discussion without supposition.
RN: I can understand your concern. The pain medications the anaesthesiologist administers during the surgery are short-acting, only a couple of hours. The anaesthesiologist will speak with you just before the surgery and you can ask more specific questions at that time. After the surgery is over, the surgical nurse will make sure Peter is comfortable and will likely give him medication for pain and swelling. You can continue this treatment when you are home with Peter. Both acetaminophen and ibuprofen are over-the-counter medications and not opioids, nor are they addictive. The surgical nurse will give you specific instructions about discharge care as well as a handout. If you don’t get this information, feel free to ask.
Rationale: In this case you respond directly to the mother’s concern about pain medication while anticipating the plan of care and other points of interface with the healthcare system. This offers reassurance about future opportunities to ask and clarify concerns. Importantly, in addition to letting the mother know what to expect, you also invite the mother to ask questions. This validates the mother’s concern and also alleviates others in the event they do not provide information.
Client’s mother: Ok, that’s reassuring. I have two kids home sick from school today with the flu. Will that be an issue for Peter?
RN: It could be. Hand-washing and keeping some space from each other if possible, will be important to minimize the spread of germs. Peter will be more susceptible to getting sick after surgery.
Rationale: This explanation responds directly to the mother’s question and offers strategies to reduce the risk of spread of germs. The response is also in everyday language, free from professional jargon.
Client’s mother: Oh boy, I’ll try.
RN: Tell me about your support system to help you manage at home.
Client’s mother: I have a good support system. My sister is really helpful with the kids, and she’s in town to give us a hand.
Rationale: In the context of this case scenario, this question assesses interpersonal relations by asking about support systems for managing this situation.
RN: That sounds like a helpful support. Are there other resources that would be helpful to you?
Rationale: This question helps assess the contextual relations through the identification of resources, and contextual issues that may require attention in this scenario. It invites further discussion about factors to consider in Peter’s care and sheds light on context for the dyad.
Client’s mother: Well the thing is that this has all come at a difficult time. I’m transitioning jobs, so money is tight right now. I don’t have extra room in the budget for a sitter. I’m glad my sister is coming, I just don’t know how long she can stay. I guess my parents could help in a pinch, but they are getting older and the kids are a lot for them to manage. And poor Peter has been sick so much lately. On one hand, I’m glad Peter will be getting the surgery to prevent other cases of strep throat, but I also feel badly that this is happening at such a stressful time for everyone. And I’m worried about the recovery time.
RN: I can see how that would be stressful. It’s going to take a few days for Peter to recover. The important thing will be to avoid the spread of germs as that could extend his recovery time. And you’re right that this surgery should help reduce his risk for getting strep throat in the future. It sounds like you have some alternative ideas for support to help you manage the recovery.
Rationale: This response offers empathy and encouragement by acknowledging what the client’s mother has shared and their support system. It also offers strategies to minimize recovery, which seems to be a concern identified by the mother.
Client’s mother: I do. Thanks.
A relational care approach attends to the broader social context in which clients and their support systems are situated (Doane & Varcoe, 2015). Also, as the nurse, you should be aware of yourself and how you influence, and are integrally connected to, the client and the healthcare system (Doane & Varcoe, 2015). This approach is an especially helpful tool for family-centred care. It also requires skill and knowledge because it demands active listening and critical thinking. Unlike closed-ended checklists, you cannot predict how the conversation will unfold.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=100#h5p-11
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=100#h5p-12
16
It is important for nurses to embody an anti-racist approach to communication. In order to do so, you need to first understand the concepts of race and racism.
Race has been systemically and historically constructed as a variable of difference, whereby people are ascribed to designated groups based on biology, culture, and/or other characteristics (Bakan & Dua, 2014). Racism is the ideology and practice of sustaining, maintaining and reinforcing difference based on race (Bakan & Dua), and it results in racialized persons being excluded from everyday points of access because of their race.
Anti-racism is the active process of changing attitudes, beliefs, practices, and policies with the goal of dismantling systemic hierarchy and oppressive power (Alberta Civil Liberties Centre, ND). An anti-racism approach involves:
The focus of anti-racism is acknowledging and working to address power inequities and systemic bias predicated on race as well as unearned privilege that is afforded to non-racialized people. Linked with racism is the concept of white privilege which refers to advantage afforded to those who are to non-racialized over persons of other racial backgrounds. It does not mean that every white person is rich, healthy, or living a lavish life. In a paper entitled “White Privilege: Unpacking the Invisible Knapsack”, McIntosh (2003) lists several daily occurrences that are privileged based on race. For example, when applying for a mortgage, skin colour will not bias financial credibility when non-racialized people are applying, but it can be a significant determining factor for those of other races. Recognizing white privilege can often be conflated with feeling guilty about race, but this is not the aim. The focus on individual guilt deviates the conversation and intention of anti-racism, which is ultimately to dismantle racist structures that subjugate and discriminate against racialized people.
Nurses play an important role in adopting and embodying an anti-racist way-of-being within their respective institutions. As a nurse, you must take an anti-racist approach in your practice and advocate on behalf of your clients when you see racism. As such, communication is essential to demonstrating anti-racism. It often begins with self-reflection and consideration for the perspective of others. See Case Study 3 for an example of an anti-racist approach to communication related to a racialized client.
Case Study 3
A nurse (RN1) receives report from a colleague (RN2). During the night shift, a client was admitted for generalized abdominal pain, and elevated blood pressure and heart rate. At this time, the etiology is undetermined, but the client is scheduled for a CT scan shortly.
RN 2: Hi Rita, it was a pretty quiet night. We just admitted a patient, I can’t even pronounce her name, in bed 2, for generalized pain. She says it is in her abdomen, but who knows what is going on. She’s giving me a lot of attitude, you know how it can be. If you ask me, I think we should have sent her home and told her to come back if things get worse.
RN1: Why is that?
Rationale: RN1 recognizes that there may be some underlying racist attitudes, and attempts to open up the conversation.
RN2: Well you know how these people are … they come to emerg for every little complaint, over-dramatizing everything. They don’t care about the costs of a visit to the emergency room.
RN1: Lorna, I’m uncomfortable with you referring to this patient as ‘these people’. Your tone and choice of words insinuates that because of how the client looks and their culture that we should dismiss their complaints about pain.
Rationale: RN1 states how they feel using “I” statements and specifically refers to the racist language that RN2 used. RN1 also uses direct language to identify passive actions of RN2.
RN2: Oh no, that’s not what I meant, I am not a racist, I was not trying to say it like that. I just meant that some people are more likely to take advantage of free health care than others.
RN1: I know this might be a difficult conversation to have, but referring to a client as “these people” and “taking advantage of the system” is racist, especially since you have attached it to the patient’s race and culture.
RN2: But that’s not what I meant.
RN1: It might not be what you meant, but the words you chose and the meaning are racist, and not acceptable. Considering our conversation, it would be good that I request our manager to organize a workshop for all of us about racism and language. Additional training will illuminate how language and beliefs like “taking advantage” are micro-aggressions that become pervasive and ultimately lead to poorer treatment and access to healthcare for racialized clients. It’s important to reflect on our communication skills and ensure we are not using oppressive language in our workplace.
Rationale: RN1 is very clear in identifying the communication as racist, but also doing so a respectful way. Even RN1’s language in inclusive in terms of the group responsibility when referring to “our” workplace.
Summary
It is important to embody an anti-racist approach to communication. It often begins with self-reflection and consideration of other peoples’ perspectives. This approach involves an active process of changing attitudes, beliefs, practices, and policies with the goal of dismantling systemic hierarchy and oppressive power. As a nurse, you must acknowledge and work to address power inequities and systemic bias predicated on race as well as unearned privilege that is afforded to non-racialized people.
17
Key Takeaways
18
Alberta Civil Liberties Centre, ND
Assembly of First Nations. (1994). Breaking the silence: An interpretive study of residential school impact and healing as illustrated by the stories of First Nations individuals. First Nations Health Commission.
Bakan, A. & Dua, E. (2014). Introducing the questions, reframing the dialogue. In A. Bakan & E. Dua (Eds.), Theorizing anti-racism: Linkages in marxism and critical race theories. University of Toronto Press.
Barnlund, D. C. (1970). A transactional model of communication. In K. K. Sereno & C. C. Mortensen (Eds.), Foundations of communication theory (pp. 83–92). Harper and Row.
Brave Heart, M. (2003). The historical trauma response among Natives and its relationship with substance abuse: A Lakota illustration. Journal of Psychoactive Drugs, 35(1), 7-13.
Centre for Addiction and Mental Health (n.d.). Trauma. https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/trauma
Chrisjohn, R., & Young, S. (2006). The circle game: Shadows and substance use in the Indian residential school experience in Canada. Theytus Books.
College of Nurses of Ontario (2019a). Practice standard: Code of conduct. https://www.cno.org/globalassets/docs/prac/49040_code-of-conduct.pdf
College of Nurses of Ontario (2019b). Practice standard: Ethics. https://www.cno.org/globalassets/docs/prac/41034_ethics.pdf
De Dreu, C., & van Knippenberg, D. (2005). The possessive self as a barrier to conflict resolution: Effects of mere ownership, process accountability, and self-concept clarity on competitive cognitions and behavior. Journal of Personality and Social Psychology, 89(3), 345-357. https://doi.org/10.1037/0022-3514.89.3.345
Doane, G., & Varcoe, C. (2015). How to nurse: Relational inquiry with individuals and families in changing health and health care contexts. Wolters Kluwer.
Ellis, R., & McClintock, A. (1990). If you take my meaning: Theory into practice in human communication. Hodder Arnold.
Health Council of Canada. (2012). Empathy, dignity, and respect: Creating cultural safety for Aboriginal people in urban health care. https://healthcouncilcanada.ca/files/Aboriginal_Report_EN_web_final.pdf
Lavallee, L., & Poole, J. (2010). Beyond recovery: Colonization, health and healing for Indigenous People in Canada. International Journal of Mental Health and Addiction, 8(2), 271-281.
Mash, T., Coholic, D., Cote-Meek, S., & Najavits, L. (2015). Blending Aboriginal and Western healing methods to treat intergenerational trauma with substance use disorder in Aboriginal peoples who live in Northeastern Ontario, Canada. Harm Reduction Journal, 12, Article 14.
McIntosh, P. (2003). White privilege: Unpacking the invisible knapsack. In S. Plous (Ed.), Understanding prejudice and discrimination (p. 191–196). McGraw-Hill.
O’Neill, L., Fraser, T., Kitchenham, A., & McDonald, V. (2018). Hidden burdens: A review of intergenerational, historical and complex trauma, implications for Indigenous families. Journal of Child & Adolescent Trauma, 11(2), 173-186.
Registered Nurses’ Association of Ontario (2007). Healthy work environments best practice guidelines: Professionalism in nursing. Registered Nurses’ Association of Ontario. https://rnao.ca/sites/rnao-ca/files/Professionalism_in_Nursing.pdf
Schramm, W. (1997). The beginnings of communication study in America. Sage Publishing.
Trauma-Informed Practice Guide (2013). http://bccewh.bc.ca/wp-content/uploads/2012/05/2013_TIP-Guide.pdf
II
By Jennifer L. Lapum, Oona St-Amant, Michelle Hughes, Joy Garmaise-Yee
19
By the end of this chapter, you will:
20
Therapeutic communication is at the foundation of the nurse-client relationship as reflected in Figure 2.1. It is different than the conversations you have with friends, peers, family, and colleagues. Therapeutic communication has a specific purpose within the healthcare context. It is intended to develop an effective interpersonal nurse-client relationship that supports the client’s wellbeing and ensures holistic, client-centred, quality care.

Figure 2.1: Therapeutic relationship.
The word “therapeutic” is related to the word therapy: it means having a restorative and healing effect on the mind and body as well as doing no harm. It is important to consider how you communicate and how this affects the client.
Points of Consideration
Learning Therapeutic Communication
Therapeutic communication is a learned activity that requires knowledge and continued practice and self-reflection.
In this chapter, you will first learn about nurses’ accountability related to therapeutic communication, and then you will learn about the principles, approaches, and strategies used in therapeutic communication in the context of a client interview.
21
Nurses are accountable to develop an effective nurse-client relationship. Therapeutic communication is one of four standard statements in the Therapeutic Nurse-Client Relationship: it is used to “establish, maintain, re-establish and terminate the nurse-client relationship” (College of Nurses of Ontario [CNO], 2019a, p. 5).
In your new role as a nursing student and your future role as a registered nurse, you must be aware of the CNO (2019a) indicators of therapeutic communication and understand your role in meeting this standard: Therapeutic Nurse-Client Relationship, Revised 2006.
For example, the indicators specify how to introduce yourself, how to refer to the client, and how to communicate with the client. You are legally obligated to practice in accordance with the CNO standards, or nursing standards in your region.
Throughout this chapter, you will learn to apply and interpret these indicators in the context of nursing practice and the client interview.
22
The client interview is an important component of nursing practice and involves several sources as reflected in Figure 2.2. It involves communicating with the client – who is considered the primary source – to collect subjective data (i.e., information that the client shares with you or the client’s family/friends). The client interview may also involve collecting data from secondary sources such as family, friends, care partners, and other healthcare providers. It is part of your assessment in which you learn about the client and combine these collected data with objective data (information that you collect when performing a physical exam).
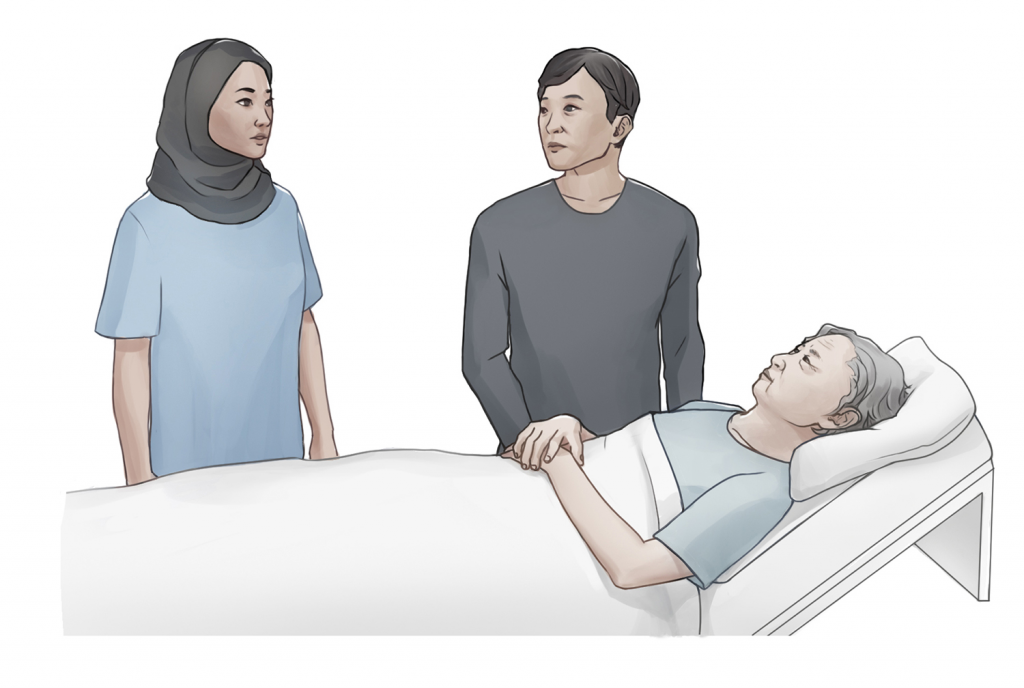
Figure 2.2: Interview sources.
As a nurse, you must ensure that the client interview is informed by the CNO (2019) Standard on Therapeutic Nurse-Client Relationship, because therapeutic communication and relationships are the foundation of an effective client interview. To meet this standard, you must think carefully about how to communicate while conducting the client interview.
The importance of good communication cannot be overstated. It is a foundational pillar of a good interview. The interview often serves as the impetus for therapeutic action. For example, without a client disclosing chest pain, it would be difficult for you to interpret what is wrong or ailing the client. The care provided by nurses is contingent on the accuracy of the data they collect, so nurses must develop their relational skills to accurately and holistically gather useful data from clients. If data are lacking, nurses are limited in providing effective care. For example, clients may not share certain problems if they are unsure whether you care or are interested. Also, clients may be afraid to reveal relevant health information because they fear judgment or ridicule, which could impede your ability to address their health issue.
The nature of the interview is influenced by the interview purpose. For example, an interview may be short and focused, or it may be more detailed and comprehensive, depending on the client’s health needs/reason for seeking care. The interview purpose is often influenced by where you work, for example an acute or primary care setting. No matter what the purpose, there are common principles and strategies to incorporate when conducting the interview, as detailed in the upcoming sections.
Points of Consideration
Care partners
The term care partners refers to family and friends who are involved in helping to care for the client. They may be referred to as informal caregivers or family caregivers, but care partners is a more inclusive term that acknowledges the energy, work, and importance of their role.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=46#h5p-13
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=46#h5p-14
Content for the Points of Consideration box was adapted from:
The Complete Subjective Health Assessment by Jennifer L. Lapum, Oona St-Amant, Michelle Hughes, Paul Petrie, Sherry Morrell, and Sita Mistry, licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
23
You should review the client’s existing health record/chart (if applicable) so that you have a general overview of the client’s main health needs/reason for seeking care and health history. If the client is already admitted, this review will not only give you an overview of the health history, but also their last 24 hours. This is an important first step for several reasons:
You should also consider how to leverage the environment of the interview location and your position within the space. The client interview is often conducted in locations such as clinic rooms, hospital rooms, emergency rooms, and community spaces such as the client’s home. You should attend to the following principles:
In preparation for the client interview, you must first be aware of the legislation and nursing standards concerning privacy and confidentiality. The Personal Health Information Protection Act (2004) states that clients have the right to have their personal health information kept private, and healthcare professionals are legally required to keep this information confidential. You must emphasize that client data is kept confidential and only shared with relevant members of the healthcare team directly involved in the client’s care. You may want to re-emphasize confidentiality when addressing sensitive interview topics such as trauma and violence, sexual health, and substance use. The client owns their personal health information; as a custodian of this information, you must request permission before disclosure (CNO, 2019b). However, there are certain situations where consent for disclosure is not required (e.g., “to eliminate or reduce a significant risk of harm to a person” [CNO, 2019b, p. 7]).
Points of Consideration
Abuse and neglect
In certain conditions, a nurse must disclose personal health information. You are legally required to report suspected child abuse or neglect, and elder abuse when the person lives in a retirement or a long-term care home in Ontario. You must report to a children’s aid society “if you have reasonable grounds to suspect that a child is or may be in need of protection” (Ontario Ministry of Children, Community, and Social Services, n.d.). For a client in a retirement home, you must report to the Registrar of the Retirement Homes Regulatory Authority; and for a client in a long-term care home, report to the Director at the Ministry of Health and Long-Term Care (Community Legal Education Ontario, 2019). You must also report to the College of Nurses of Ontario (2020) if a client discloses or you observe a “nurse who poses a serious risk of harm to patients” (sexual abuse, incompetent care, physical or mental incapacity to provide safe care, or professional misconduct).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=48#h5p-15
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=48#h5p-16
24
Like everyone, nurses are susceptible to stress, sadness, anger, and an array of other emotions. Despite good intentions, your communication will be strongly influenced by your mood, thoughts, and emotions. Self-reflection is an important tool for recognizing your emotional state and minimizing unintentional miscommunication with clients, i.e., non-therapeutic communication. See Figure 2.3.
Figure 2.3: Self-reflection
See Table 2.1 for strategies on how you can self-reflect before commencing the client interview.
Table 2.1: Self-reflecting on emotions and thoughts.
Reflective Practice | Consideration |
How are you feeling? | Nurses are not exempt from life circumstances that can cause uncomfortable emotions like sadness, anger, frustration, as well as other emotions such as happiness and gratefulness. While it may be impossible to put aside your emotions, having a sense of your emotions and their cause is a very powerful tool to avoid inadvertent miscommunication. |
What is occupying your thoughts? | It can be helpful to step outside of the narrative in your mind. It is not abnormal for a thought to pervade your thinking, but suspending such thoughts and being in the moment with the client can assist with better communication. Consider if something is weighing on you. Are you ruminating about an event, a person, an idea? |
In what ways are you physically expressing your emotions and thoughts? | Your emotions and thoughts are sometimes physically expressed through facial expressions, hand gestures, and body language. Can someone tell that you are happy or sad by looking at you? Being aware of the physical expression of your emotions and thoughts can assist you in your communication with others and enable you to convey emotions like empathy, compassion, and concern. |
How is your health and wellbeing? | Often physiological and psychological/emotional events like hunger, fatigue, body aches, and sadness can shape your mood. Reflect on how you are feeling in relation to your body and mind and pay attention to your body’s cues. |
What is the environment surrounding you? | Even when you think you are accustomed to the work environment, subtle triggers can affect your ability to effectively communicate. A beeping machine, foul smell, or bright lights may affect your ability to focus, show concern, and actively listen. Reflect on yourself in relation to the environment and consider what factors you can and cannot control. |
As you self-reflect, consider that the healthcare environment often intensifies emotions for clients and their families. It can be a place where people experience pain, discomfort, and stress. Clients may hear bad news and confront truths about themselves, or experience intense joy and relief. Because such extremes can exist in the healthcare space, the client is often more attune to you (the provider) than you may be aware. The client may be telegraphing your body language or intuiting your choice of words. For this reason, providers need to be self-aware and temporarily suspend their own needs in order to authentically connect with the client.
Points of Consideration
Mindfulness
Mindfulness can be a useful strategy for connecting with clients and authentically being fully in the moment as they respond. It’s easy to get caught up in the fast-pace clinical environment and be distracted by preceding events. Clients pick up on distraction and this can undermine trust.
Mindful meditation has been proven to reduce stress among healthcare professionals, including nurses. Once learned, it can be used at any time, and can improve your therapeutic communication with the client.
25
There is a standard way to begin interviews so that the client knows who you are and why you are there.
Introducing yourself and addressing the client
Begin by introducing yourself by name and category to the client, and determine how the client wants to be addressed (CNO, 2019a). Also, best practice has shifted to include your own pronouns and ask what pronouns the client uses in order to create an inclusive environment. For example, a nurse may say, “Hello, I am Mac Li Ken Ji. I am a registered nurse. Please call me Mac. My pronouns are he/him. How would you like me to refer to you and what pronouns do you use?” It is important not to use the term “preference” when referring to pronouns and gender as these are not preferences.
Because registered nurse is a protected title, you can only refer to yourself as a nurse when you are a member of the College (i.e., the College of Nurses of Ontario). If you are a nursing student, you should identify your category based on your institutional requirements. For example, you may consider identifying the year of the nursing program you are in (e.g., nursing student year one, nursing student year two, nursing student year three, nursing student year four). For example, in year one of the program, you may say, “Hello, I am Misa Rodriguez. I am a nursing student year one. I am working with your registered nurse, David, today.”
Identifying the purpose of the encounter
As per CNO (2019a), part of the introduction phase of the client interview is to identify your role, which involves the purpose of the encounter. You should also notify the client that any information collected will be kept confidential and if applicable, identify who the client’s information will be shared with. Nurses often let clients know that they will also be taking notes.
Here are some examples:
See Film Clip 2.1 and 2.2 demonstrating an effective and ineffective introduction to the patient interview.
One or more interactive elements has been excluded from this version of the text. You can view them online here: https://pressbooks.library.ryerson.ca/communicationnursing/?p=52#video-52-1
Film Clip 2.1: Effective interview introduction. (Also, consider sharing your own gender pronouns with the client and asking what pronouns they use).
One or more interactive elements has been excluded from this version of the text. You can view them online here: https://pressbooks.library.ryerson.ca/communicationnursing/?p=52#video-52-2
Film Clip 2.2: Ineffective interview introduction.
Points of Consideration
Name and category
As a nurse, you are required to introduce yourself by your first and last name and your category (College of Nurses of Ontario, 2019d). By using your full name, you relay accountability and take responsibility for your work. There are situations when nurses do not use their full name or use a pseudonym, which is permitted as long as the employer is aware and the College of Nurses of Ontario is able to identify you through your employer; for example, this is permitted when you have reasonable grounds for your safety (College of Nurses of Ontario, 2019c).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=52#h5p-17
26
There are three types of questions that guide the client interview.
Figure 2.4: Types of interviewing questions
Closed-ended questions are direct questions that you ask when you are seeking precise information. These types of questions typically generate a short answer and do not facilitate a dialogue. Here are some examples in which the answers are typically one word:
Open-ended questions are types of questions that invite the client to share descriptive answers, open up about their experience, and answer in a way that is most relevant or comfortable from their perspective. In response to open-ended questions, clients typically talk in sentences and may even tell stories (as opposed to the short answers to closed-ended questions). Although clients may provide a short answer, this type of question still provides the opportunity for you to probe further. Here are some examples:
You should listen to the answer carefully so that you can authentically respond to what the client said and possibly probe further.
Probing questions are types of questions and statements that allow you to gather more subjective data based on a client’s response. These types of questions can also be used to summarize and clarify a client’s response or resolve discrepancies that you identify. These questions and statements can be open- or closed-ended. Here are some examples:
Points of Consideration
Learning how to respond
Sometimes you won’t know how to respond when a client says something. For example, they may say something that you don’t understand or something that surprises you or takes you off guard. You may consider responding with statements like, “Tell me more” or “Tell me more about what you mean by that.” Avoid statements that may conjure judgement such as “why” or “how come” – these statements can be interpreted as a demand for an explanation and make the client feel defensive.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=54#h5p-18
27
There are many communication strategies that should be used to facilitate therapeutic communication. See Table 2.2 for a list of these strategies and considerations and examples on how they build the therapeutic relationship.
Table 2.2: Communication strategies.
Strategy | Considerations and Examples |
Use clear and simple language so the client understands what you are saying. | It is best to avoid or limit medical and professional language that clients may not understand. Remember, knowledge is power; when you use language that others may not understand, it can reinforce subordination and exclusion. By speaking simply and clearly, you include clients regardless of their professional or educational point of reference.
|
Be an active listener. Active listening is a type of listening that shows you are engaged in the conversation and that you hear and understand what the client is saying. Active listening is important to facilitate your understanding of, and the integration of, client’s experiences, preferences, and health goals into their care. | You might show that you are an active listener by using eye contact and having an open posture. You can also use facilitation strategies that show active listening, and also encourage the client to elaborate such as, nodding, and responding by saying “uh huh” and “tell me more.” Active listening can also be demonstrated by paraphrasing what the client says, which shows that you are listening and encourages them to elaborate. |
Use silence. Silence is a strategy that aids active listening. It can be beneficial in situations where the client is talking about something personal or is struggling to find the words for what they want to say. Clients may also need time to think and reflect after you have asked a question. | Sometimes silence can be uncomfortable, and professionals want to fill the void with words. It is better to show interest and understanding and give the client time to think about how they best want to say what they want to say. If the client seems to be feeling awkward about taking too much time to think, you can say “It’s ok. Take your time.” |
Be empathetic. Empathy is the action of understanding another person’s emotions and experiences while suspending your own viewpoint. You have probably heard the phrases “put yourself in someone else’s shoes” or “see the world through the eyes of another person.” Being empathetic helps the client feel understood and cultivates a trusting and therapeutic relationship. | It is important to imagine what another person is experiencing. You need to be curious and demonstrate interest by responding to what the client is saying (e.g., “Tell me more. How do you feel about it?”). Don’t get caught up in following your interview guide – it’s important to let the client’s narrative shape the interview. When a client is talking about a difficult experience, you may say something such as, “That must be very difficult.” |
Be honest. Part of therapeutic communication involves being authentic and truthful. In order to do so, you should be straightforward with clients while also talking to them in a compassionate manner. If you are talking about a difficult or emotionally laden topic, demonstrate compassion by sitting down, maintaining eye contact, and being aware of your vocal intonation. | Part of being honest involves avoiding false reassurance. False reassurance is when you assure or comfort the client about something that is not based on fact. When someone voices fear or anxiety, people tend to automatically respond by assuring them that everything will be okay. An example of false reassurance is when the nurse says, “it will be okay” when a client says, “I am scared I might die.” This kind of response is not honest and does not open up communication. It is more effective and honest to say, “tell me more.” See Film Clip 2.3 demonstrating false reassurance and Film Clip 2.4 on how to avoid false reassurance. You should also avoid distancing and avoidance language. Distancing is when you attempt to create a false space/distance between a threat and the person (e.g., “the cancer has spread to your brain” as opposed to “your cancer…”). Avoidance language is unclear language (e.g., “your partner didn’t make it” or “they are now at peace”). It’s better to use specific language (e.g., “your partner died”). Being direct demonstrates honesty and ensures clarity for the client. |
Demonstrate unconditional positive regard, which means accepting and respecting that each client has agency to believe and behave how they want, or feel is best. You don’t have to agree or approve, but your acceptance of their self-determination should not be conditional on its alignment with your beliefs or behaviours. | Using this approach involves accepting that clients are generally doing the best they can. Avoid judging or blaming them for their beliefs, behaviours, or conditions. You should avoid questions that begin with “why” as this can imply blame. For example, avoid “why do you smoke?” You can reframe this inquiry as, “tell me about the reasons that you smoke.” |
Use permission statements to open conversations that may be difficult to talk about. Permission statements are a combination of statements and questions that suggest to the client that an experience or feeling is expected or normal. | One example of a permission statement is: “Often, children your age experience changes in their body that they have questions about.” Another example is: “Clients that have experienced your type of surgery often have questions about sex. Do you have any questions for me?” Another example is: “Many people your age begin to experience problems with urinary incontinence, have you had any issues?” |
Ask one question at a time so that the client understands it and so that you are more likely to receive a clear answer. | You should avoid asking multiple questions at once because this can be confusing for clients. Here is an example: “Tell me about your support system. Your brother seems like he’s a great help, right? Do you have anyone else to support you?” Instead, try it this way to start: “Tell me about your support system?” – then, wait for an answer. You can probe with follow-up questions depending on what the client says. |
Be conscious of how your vocal qualities influence nurse-client communication. Vocal qualities refer to intonation, speed, and rhythm. | These vocal qualities influence the communication process in terms of the emotions you convey and your interest in the conversation, as well as how a client interprets what is important. For example, speaking quickly can be interpreted as the nurse being in a rush to leave. |
Work collaboratively with the client during the interview so that they are an active agent with self-determination. By using a relational inquiry approach and working collaboratively, you can focus on what is important to the client. | Part of focusing on what is important to the client involves providing information that they identify as relevant to them. Avoid being authoritative and giving unwanted advice, but it’s a good idea to ask if the client is interested in learning more about a topic. |
One or more interactive elements has been excluded from this version of the text. You can view them online here: https://pressbooks.library.ryerson.ca/communicationnursing/?p=56#video-56-1
Film Clip 2.3: Demonstration of false reassurance.
One or more interactive elements has been excluded from this version of the text. You can view them online here: https://pressbooks.library.ryerson.ca/communicationnursing/?p=56#video-56-2
Film Clip 2.4: Demonstration of how to avoid false reassurance.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=56#h5p-19
28
Non-verbal communication strategies are ways you communicate without speaking, for example through facial expressions, hand gestures, eye contact, and body language. See Figure 2.5.

Figure 2.5: Non-verbal communication
In many situations, much of your communication occurs through non-verbal behaviours. Non-verbal communication can be a useful strategy for communicating emotions like empathy, compassion, and acceptance. It is often how nurses respond, rather than what they say, that leaves a lasting impression on clients, so it is important to be aware of how you communicate using non-verbal behaviours.
Non-verbal behaviours must align with your verbal behaviours so that clients clearly understand what you are saying. For example, it would be confusing for the client if you had a somber tone of voice, distancing posture, and avoided eye contact while attempting to maintain a therapeutic relationship with the client.
Try to ensure positioning where you are both at the same vertical level and a slight angle towards one another. This positioning conveys an open and non-confrontational and non-authoritative space. Whenever possible, avoid standing over the client if they are sitting or lying in bed. It is better to sit down, which also conveys that you have time to listen to them.
There are many models to inform your non-verbal communication. One helpful model is called SURETY (Stickley, 2011) reflected as a modified version in Figure 2.6:
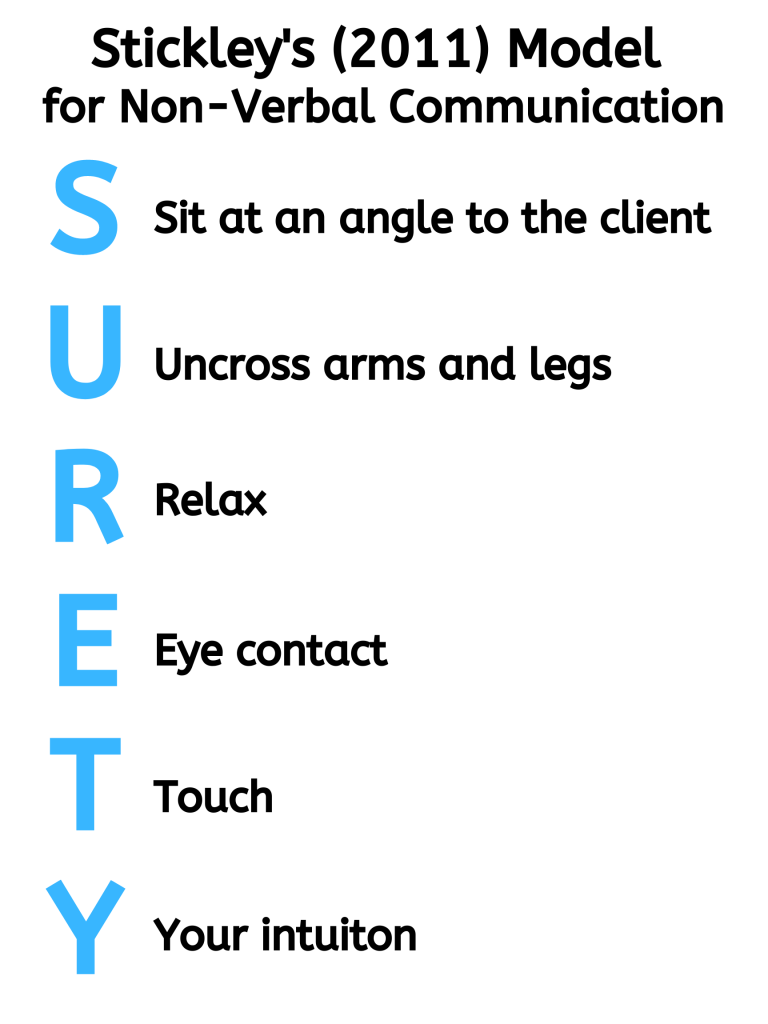
Figure 2.6: The SURETY model.
Points of Consideration
Physical touch
Touch can be therapeutic with clients when used appropriately. It can convey empathy and compassion. You should strike a balance about when it is therapeutically appropriate and when it is an intrusion for clients. It will take practice to learn when touch is appropriate.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=58#h5p-20
29
Therapeutic communication with clients and families requires attention to a person’s culture. It is important to note that:
Cultural safety is an important component of therapeutic communication, because culture is so dynamic and deeply embedded in a person’s way of being. In the context of therapeutic communication, you must examine your own culture and how it affects the ways you communicate with clients. This self-awareness is vital to provide culturally safe care to clients and facilitate health equity (Curtis et al., 2019).
A relational approach can facilitate communication that embraces cultural safety because it relies on your dialogical engagement with the client. In other words, nurses should suspend what they assume they know about culture, and let clients direct nurses with regard to how culture is meaningful to them. This approach encourages you to consider the relational interplay (Doane & Varcoe, 2015) of communication, the client’s culture, and your own culture. Like everyone, nurses are cultural beings with ethnocentric tendencies – you will tend to view the world and your client from your own cultural perspective. From a relational perspective, you must understand your own culture and your ethnocentric tendencies so that you are positioned to recognize and understand the client’s culture.
Part of a relational approach also involves positioning yourself as an inquirer who is in a “space of knowing/not knowing, being curious, looking for what seems significant” (Doane & Varcoe, 2015, p. 6). See Table 2.3 on how to develop yourself as an inquirer and understand the interplay of your culture and the client’s culture.
Table 2.3: Understanding culture.
Your Own Culture | The Client’s Culture |
How do you define your culture? What does a typical day involve for you? How does your culture affect your health and illness? What are your own biases, attitudes, prejudices that may affect how you care for and communicate with the client? If you were in the client’s shoes, what would be important for you to share with your nurse about your culture so that they could better care for you? | Tell me about your culture. Tell me about a typical day for you. Tell me about what is important to know about your culture in order to care for you best. How can I provide care to you that is culturally safe? |
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=60#h5p-21
30
A person’s age needs to be considered when conducting the client interview. Most importantly, you need to consider a client’s developmental stage. Developmental stage does not always align with a client’s chronological age. With regard to communication, a focus on developmental stage includes attention to areas such as language and cognitive and socio-emotional development. At times, you may need to modify your communication so that you are appropriately engaging with the client at a level they understand.
There are many ways to construct chronological age categories. Broadly, children are considered anyone under 18 and adults are considered anyone 18 and older. More specifically, you could consider the categories used in this resource:
See Film Clip 2.5 of an expert pediatric nurse speaking about how communication varies between children and adults.
One or more interactive elements has been excluded from this version of the text. You can view them online here: https://pressbooks.library.ryerson.ca/communicationnursing/?p=62#video-62-1
Film Clip 2.5: Interview with an expert pediatric nurse.
The following sections provide tips on broad chronological age categories including young children, older children and adolescents, and adults including older adults.
31
You should use a combination of verbal and non-verbal communication with infants. Be constantly aware and adapt your use and choice of communication strategies based on the infant’s response.

Figure 2.7: Young children
Most infants enjoy hearing the human voice, and this is how they learn and make sense of language. You should talk to them in a relaxed and pleasant tone of voice even though they cannot verbally respond. It’s also okay to use baby talk with infants as it can help with language development: baby talk is a type of speaking where you use enhanced vocal intonation and hyperarticulation of sounds such as vowels and consonants.
In terms of non-verbal communication, you should have a relaxed body posture, smile, use appropriate eye contact, and gestures with your hands; these techniques are important with all children because non-verbal language can facilitate their sense of safety.
With children, you should adapt your communication to their developmental stage. Tailor your language to a level that children will understand, avoiding long complex sentences and instead using short sentences with simple words. Although you may use baby talk with infants, you should use a different approach with toddlers, who often want to be included in the conversation. As children get older, they enjoy receiving compliments and encouragement to connect with them (e.g., “look how much you have grown” or “great job!”).
Because care partners (typically parents) are usually present with young children, it’s important to involve them so that the child feels safe. Here are some points to consider with care partners:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=64#h5p-33
32
Older children and adolescents are usually at a stage where they can participate in the client interview in a more active way and articulate their experiences, emotions, and needs. Thus, it is important to address them as the client first, as opposed to the care partner. Care partners are often still involved, but you should offer the child/adolescent the opportunity to speak with you privately at times. For example, you might say to the client: “At this age, I often like to provide time to speak with you alone. Are you okay if I ask your mom or your dad to step out for a few minutes?”
You should continue to use a combination of non-verbal and verbal language and communication strategies. In terms of non-verbal communication, use eye contact with a relaxed and open posture that demonstrates interest in what they are saying. Smiling may be appropriate depending on the topic. You should also facilitate the interview using strategies such as nodding and statements that encourage the client to continue sharing (e.g., “uh huh” and “tell me more”). Be aware of your facial expression and vocal intonation to ensure you are conveying empathy, acceptance, and a non-judgmental attitude. You may want to include fun objects or games, or include the child in the assessment process (e.g., “would you like to try tapping on your own knee with this reflex hammer?”).
Adolescents are in a transitional stage where they are still children but are moving closer to adulthood. It is important to recognize and respect their self determination. Additionally, emotional and cognitive capacity will vary from adolescent to adolescent and from situation to situation. Therefore, your communication strategies will need to shift based on the adolescent and the situation. Overall, you should convey acceptance, honesty, and respect. Avoid talking to them as a child, as this is often interpreted as demeaning. Some adolescents are old enough to make their own decisions regarding some aspects of their health care: in many jurisdictions, this capacity to consent, which includes being able to understand and weigh risks and benefits, is determined by maturity level rather than by age.

Figure 2.8: Adolescents
When discussing sensitive and intimate topics, it is important to recognize that adolescents often feel self conscious, embarrassed, and have a fear of being judged. Your communication strategies should convey acceptance and understanding of what they are experiencing. You should have an open and non-judgmental attitude so that you can cultivate a trusting relationship with the client. Permission statements can be particularly useful as they can help normalize what an adolescent may be experiencing.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=66#h5p-24
33
Adulthood is a large age category including everyone 18 years and older, but there is great diversity within this group. Some adults will have had minimal encounters with nurses and others will have had extensive encounters. Younger adults in their late teenage years and early twenties may share characteristics with adolescents, so you may use many of the same communication strategies. You should also examine and acknowledge your own biases and tendencies to stereotype older adults and constantly re-assess your own assumptions so that they do not negatively affect your communication.

Figure 2.9: Adults and older adults.
With older adults, it is important to give them time to process and answer questions, as they may have a slower response time. Avoid making assumptions about their hearing or vision or cognitive capacity. Rather, speak in a clear voice and face them while you speak as you would with all clients. It can be helpful to write down instructions or educational information for older adults, as they are often dealing with substantial quantities of health information.
Some older adults may have a care partner present with them because they are managing multiple illnesses and may have cognitive or physical impairments that cause disabilities. When a care partner is present, you should engage in an inclusive communication approach. After engaging in the introductory phase with the client, ask about who the person with the client is. If appropriate, you should consider the client and care partner as a dyad in which both are recipients of care, but the client should be your main focus during your assessment. Avoid assuming that care partners can better answer questions for older clients. For example, direct your questions to the client even though the care partner may help answer some of the questions.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=106#h5p-25
34
As a nurse, you will encounter other populations and situations that will require you to thoughtfully consider how to best communicate in a way that is respectful, effective, and therapeutic. You might not even know when you are caring for certain populations, because it may not be obvious, so it is always best to ground your communication in best practices (e.g., College of Nurses of Ontario practice standard concerning therapeutic nurse-client relationship). For example, it is not necessarily readily apparent when a language discordance exists, or when a person is experiencing intense emotions, or when a person has a disability.
Language discordance
There will be times when you and the client and/or family do not speak the same language. In this case, you need to carefully assess and evaluate their understanding.
Here are some strategies to address language discordance:
Emotions
Clients commonly experience sadness, anger, fear, anxiety, embarrassment, and other emotional responses in the context of health and illness. It is important that you cultivate a therapeutic environment where clients feel comfortable to open up about their emotions. Open-ended questions like “Tell me about how you are feeling” can facilitate discussions about a client’s emotional response. Additionally, you might consider using permission statements to help normalize how the client is feeling and provide an opening for them to speak about emotions. For example, “Clients often experience sadness or anger when they are diagnosed, how are you feeling?”
It is important that you acknowledge the client’s emotions and provide space for them to experience the emotions. Avoid changing topics. Give the client time to voice their emotions or even cry. Using silence and active listening are effective communication strategies during these circumstances.
Violence and trauma
Many clients will have experienced violence and trauma in their lives such as abuse, bullying, grief or loss of a loved one, or natural disasters or war. You will often not even be aware that they have experienced violence or trauma, so it’s best to use a trauma-informed approach with all clients, as discussed in Chapter 1. Approach all clients with the assumption that they may have experienced violence and trauma at some point in their lives. Reflect on how best to help them feel safe and provide them as much choice and control in the clinical encounter as possible.
Some communication strategies that are consistent with a trauma-informed approach include:
Communicating with clients about violence and trauma requires knowledge, skill, and experience. This field of study is vast and deep. As you develop foundational communication skills, you will have opportunities to build knowledge about trauma-informed communication. For now, recognize that there is much more to know about trauma-informed approaches and that an in-depth understanding is needed to best care for these clients.
Hearing and visual impairment
You can inquire about the presence of any hearing or visual impairment and what is best for the client in terms of communication. For people with hearing and visual impairment, begin by minimizing any background noises or distractions. You should speak in a clear, slightly louder voice, steady tone with a deeper pitch. Avoid shouting and using a high pitch as this can distort sounds and make your words more difficult to hear. You should face the client directly and clearly articulate your words so that they can read your lips and attend to non-verbal cues as necessary. If the client has an assistive device (e.g., glasses or a hearing aid), make sure that they have access to the device.
Intellectual impairment
Some of your clients will have intellectual or cognitive impairments that may result in disabilities affecting their ability to learn and reason (e.g., Down syndrome, fetal alcohol syndrome). You should consider how each client can best participate in communication (e.g., listening, talking, understanding and processing information). You should engage in active listening and determine what is important to the client. Speak clearly and ask simple questions. Speak in a positive tone with a steady pace and avoid speaking slower as this can come across as patronizing. You may encourage them to bring someone with them that they trust, such as a care partner; you should still focus your attention on the client but also create an inclusive space for the care partner to be involved.
Substance impairment
A client under the influence of drugs and substances (alcohol, cannabis, prescribed medications, and/or illegal street drugs) can have altered capacity to think, reason, and communicate. Although some of these substances may be illegal and non-prescribed, it is important to maintain a non-judgmental attitude and convey unconditional positive regard. As a nurse, it is not your job to judge a client. Rather, you should use a relational inquiry approach to understand the circumstances that have influenced their choices and respect that each client has agency and self-determination.
While the client is under the influence of a substance, use communication strategies that facilitate their capacity to understand what you are saying and communicate with you while maintaining safety. Thus, you should speak clearly and in short simple sentences. Focus on the reason for seeking care or the priority issue. There will be time for a collaborative discussion and health promotion after the effects of the substances have dissipated.
Escalation
Communication is a particularly important strategy to use when your purpose is to de-escalate a situation. Escalation can occur in any healthcare situation when clients are encountering intense emotions and experiences entangled with stress, fear, anger, uncertainty, pain, and lack of control. This can lead to the client spiraling out of control, agitation, aggression, and even violence. Contextual factors may include clients who have received bad news such as a diagnosis, clients who are under the influence, and/or clients who are having a mental health crisis. Attend to your own safety and be aware of the potential risk factors. It is important to notify a colleague(s) when interviewing a client who is at risk of, or has a history of, escalating.
De-escalation includes ways to reduce and/or prevent escalation. De-escalating communication strategies include:
Inappropriate communication from the client
There will be times when clients engage in inappropriate communication. This kind of communication may include verbal and non-verbal language such as inappropriate physical touch, violent or aggressive behaviour, harassing language (e.g., name-calling, threats), and sexualized language. As a nurse, you should rely on the CNO (2019a) practice standard about the therapeutic nurse-client relationship. Keep in mind that there is meaning associated with all client behaviour and that you should attempt to understand it (CNO, 2019a).
Consider these strategies when responding to inappropriate client language:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=108#h5p-26
35
Concluding the interview has three main purposes:
As part of the conclusion, you should provide a brief summary of the data you have collected. This summary should reflect what the client said and may include paraphrasing what they said. You might start the summary off by saying “The interview is coming to a close and I would like to share a summary of what we discussed.” The length of the summary will depend on the comprehensiveness of the interview and the complexity of the client’s needs, but it is usually a few sentences summarizing the pertinent data. This can be followed up by a couple of questions such as “Did I capture what you said accurately?” and “Is there anything else that you would like to share with me that is important to your care?”
Finally, you should discuss the next steps related to the client’s care. For example, these may include a physical assessment or having another health professional come in to talk with them. Make sure you ask the client if they have any questions before concluding the interview. Finally, close the interview in a therapeutic way, which may involve using the name that they prefer to be called and thanking them for sharing their information.
36
Key Takeaways
37
College of Nurses of Ontario. (2020). What to report. https://www.cno.org/en/protect-public/employers-nurses/reporting-guide/what-to-report/
College of Nurses of Ontario. (2019a). Therapeutic nurse-client relationship, revised 2006. https://www.cno.org/globalassets/docs/prac/41033_therapeutic.pdf
College of Nurses of Ontario. (2019b). Confidentiality and privacy – personal health information. https://www.cno.org/globalassets/docs/prac/41069_privacy.pdf
College of Nurses of Ontario. (2019c). Professional conduct: Professional misconduct. https://www.cno.org/globalassets/docs/ih/42007_misconduct.pdf
College of Nurses of Ontario (2019d). Code of Conduct. https://www.cno.org/globalassets/docs/prac/49040_code-of-conduct.pdf
Community Legal Education Ontario. (2019). When does elder abuse have to be reported? https://www.cleo.on.ca/en/publications/elderab/when-does-elder-abuse-have-be-reported
Curtis, E., Jones, R., Tipene-Leach, D., Walker, C., Loring, B., Paine, S., & Reid, P. (2019). Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. International Journal for Equity in Health, 18(1). https://doi.org.10.1186/s12939-019-1082-3
Doane, G., & Varcoe, C. (2015). How to nurse: Relational inquiry with individuals and families in changing health and health care contexts. Wolters Kluwer.
Kashima, Y. (2019). What is culture for? In D. Matsumoto & H. Hwang (Eds.), The handbook of culture and psychology (2nd ed., pp. 123-160). Oxford University Press.
Kim, U., Park, Y-S., & Park, D. (2000). The challenge of cross-cultural psychology: The role of Indigenous psychologies. Journal of Cross-Cultural Psychology, 31, 63-79. https://doi.org/10.1177/0022022100031001006
Ontario Ministry of Children, Community, and Social Services. (n.d.) Reporting child abuse and neglect. http://www.children.gov.on.ca/htdocs/english/childrensaid/reportingabuse/index.aspx
Personal Health Information Protection Act. (2004). https://www.ontario.ca/laws/statute/04p03
Stickley, T. (2011). From SOLER to SURETY for effective non-verbal communication. Nurse Education in Practice, 11, 395-398. https://doi.org/10.1016/j.nepr.2011.03.021
III
By Jennifer L. Lapum, Charlotte Lee, Michelle Hughes, Oona St-Amant, and Joy Garmaise-Yee
38
By the end of this chapter, you will:
39
Interpersonal communication can be defined as the process of exchanging messages between people whose lives mutually influence one another. This kind of communication involves two or more people who are interdependent. For example, the communication you engage in with family, friends, and peers is considered interpersonal communication, as illustrated in Figure 3.1. Interpersonal communication builds, maintains, and evolves relationships, so it is foundational to many aspects of everyday life.

Figure 3.1: Example of interpersonal communication
Interpersonal communication is interactive and structured by social expectations, including unspoken norms that are assumed or taken for granted during language exchange. These norms are often culturally influenced and contextually relevant, but although they are instituted early in life, they are not immutable – they change and evolve over time. For example, how you greet people (vocal intonation, whether you address someone by their prefix, whether you shake hands or bow) can change over the years. Furthermore, social expectations are shaped by the parties involved, so how you speak with friends will be different from how you speak with a professor, for example.
Interpersonal communication is also usually goal-oriented and fulfills instrumental and relational needs.
One type of interpersonal communication that will be important in your work as a healthcare professional is interprofessional communication. Let’s move on and explore this type of communication!
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=118#h5p-27
Adapted from:
https://open.lib.umn.edu/communication/chapter/1-1-communication-history-and-forms/
40
Within the context of health care, interprofessional communication can be defined as communication among members of a client care team, which may include members of various professional groups. For example, it may involve you as the nurse, clients, families, and also other healthcare professionals such as physicians, physiotherapists, midwives, pharmacists, dieticians, and personal support workers.

Figure 3.2: Interprofessional communication
Interprofessional communication involves verbal, written, and non-verbal communication as defined in Chapter 1.
During interprofessional communication, verbal communication may include conversations between two or more members of the interprofessional team, usually in person as illustrated in Figure 3.2 or over the telephone. See Table 3.1 for specific communication types and examples that are common in healthcare.
Written communication in the interprofessional context commonly includes documentation notes in a client’s chart such as progress notes, physician orders, medication administration record, diagnostic reports, referral letters, and discharge notes. Other examples may include faxes and emails, and more recently, texts.
Finally, non-verbal communication in the interprofessional context involves meaning and interpretation conveyed through body language such as facial expressions, eye contact, body position, and gestures. It is important to be aware of your body language and ensure that it aligns with your verbal language.
Table 3.1: Examples of interprofessional communication
Communication type | Verbal communication example |
Client/unit rounds where an interprofessional group discuss the client’s status and plan of care – many times the client and family are involved in these rounds. | Nurse: “Mr. Molina’s blood pressure has been stabilized all night with no chest pain since 2330. He remains on a saline drip and is scheduled for a cardiac catheterization this morning.” Physician: “What’s his cognitive and renal status like?” Nurse: “He is alert and oriented. No renal issues. He was started on an oral beta blocker last night and had a dose this morning, and was given a dose of 20 mg furosemide this morning too. However, he is wondering about whether he should be restarted on his cholesterol medication.” Physician: “Yes, that is fine to restart, and please notify me when his cath results come back.” Nurse: “Sounds good.” |
In-person or phone conversations in which you are providing a client update and consulting another healthcare professional on a plan of action. | Nurse: “Hello, I am Rita Lin, a registered nurse working with the client Meaka Lorne at General Highschool. Meaka is having suicidal ideation although she does not have an immediate plan. However, I think it is time to initiate more intensive therapy.” Therapist: “Yes, I remember Meaka. How is her anxiety and depression?” Nurse: “Her anxiety has been exacerbated over the last couple of weeks, and as a result she hasn’t been going to school. She has felt quite sad and gloomy over the last week, which is when the thoughts of suicide emerged.” Therapist: “I recall this is how it began last year.” Nurse: “Yes, she also indicated that.” Therapist: “Can you remind me whether she still lives with her father.” Nurse: “Yes, she does, and he is with her at home right now.” Therapist: “Okay, let’s get her in for an appointment.” |
Discussions that occur among healthcare professionals while providing client care. | Physician: “I am just about to insert the central venous catheter, could you shift the light a little this way.” Nurse: “Yes, no problem. I have the IV primed, just let me know when you want me to hand it to you.” Physician: “Will do. Ms. Bykov, you will feel a slight pinch, if you can stay still.” Client: “Okay.” |
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=121#h5p-28
41
Interprofessional communication is a fundamental component of interprofessional collaboration. Effective interprofessional collaboration fosters effective teamwork among members of an interprofessional client care team to optimize client outcomes (Canadian Interprofessional Health Collaborative, 2010), ensuring that clients are safe throughout the healthcare system (Canadian Nurses Association, n.d.a.).
Because of the significance of interprofessional collaboration, the Canadian Interprofessional Health Collaborative has developed a National Interprofessional Competency Framework, as shown in Figure 3.3.
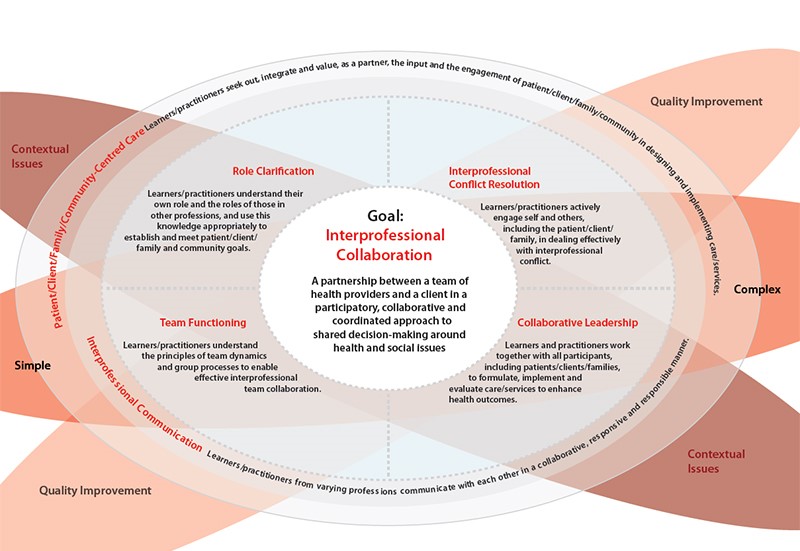
Figure 3.3: National Interprofessional Competency Framework
As shown in Figure 3.3, six interdependent competency domains have been identified to achieve the goal of interprofessional collaboration (Canadian Interprofessional Health Collaborative, 2010). These are defined as the “knowledge, skills, attitudes, and values that shape the judgements essential for interprofessional practice” (Canadian Interprofessional Health Collaborative, 2010, pg. 9) and include:
The first two competencies have a strong influencing role in all healthcare situations, so as shown in the figure, they encircle the other four competencies. This framework can assist you in contributing to effective healthcare team functioning with a focus on communication and working together collaboratively.
This chapter focuses specifically on the competency domain of interprofessional communication. This plays a central role in interprofessional collaboration because it supports the other five competency domains (Canadian Interprofessional Health Collaborative, 2010).
To fulfill the interprofessional communication competency, nurses and all healthcare professionals must develop the capacity to “communicate with each other in a collaborative, responsive and responsible manner” (Canadian Interprofessional Health Collaborative, 2010, p. 16). This means that each healthcare professional is responsible for engaging in effective communication in the specific clinical and interprofessional context in respectful, explicit, and clear ways (Lyndon et al., 2011). It is important to actively respond to the perspectives of everyone involved, including the client and other healthcare professionals. Table 3.2 presents strategies for effective interprofessional communication, adapted from the Canadian Interprofessional Health Collaborative.
Table 3.2: Strategies for effective interprofessional communication
Descriptors | Example and explanation |
“Establish teamwork communication principles” (p.16). | Example: Each homecare agency has set procedures for homecare nurses to assess heart failure clients daily through remote monitoring of vital signs, weight, intake, and output. The client may tell the nurse that they have gained a couple of pounds this week. When significant changes like sudden weight gain arise, the nurse would submit a standardized electronic form to a clerk at a cardiac outpatient clinic. The cardiologist and nurse practitioner are then immediately alerted to the request for consultation and follow-up by phone with the client’s homecare agency nurse. This ensures that unforeseen changes in client status are managed appropriately and in a timely manner. Explanation: A clear set of communication principles and procedures is important for healthcare teams that work closely together and depend on each other. These types of principles and procedures can foster open and creative discussions, recognition and appreciation of each person’s role and contribution, as well as transparency in decision-making. |
“Actively listen to other team members” (p. 16). | Example: A client is having trouble eating. The following conversation may occur. Dietician: “Let’s provide the client pureed foods to help with swallowing and reduce risks of choking.” Nurse: “I agree. I have noticed that the client needs to sit up straight and he takes a long time to chew. I will arrange for a pureed diet, should we also thicken any fluids?” Dietician: “Yes.” Nurse: “Okay, Mr. Rhoda, would you like to try some apple sauce to start?” Client: “Yes, please.” Explanation: Active listening involves closely attending to what another person is saying and responding to them based on what they said. |
“Communicate to ensure common understanding of care decisions” (p. 16). | Example: When giving a sponge bath, a nursing student notes reddened skin at the lower back of the client. The nursing student discusses the finding with their preceptor and personal support worker. The preceptor informs the nursing student that the client likely has a stage 1 pressure ulcer and should be turned frequently according to institution policy. The nursing student confirms the need and reason for frequent turns and reiterates the need for good hydration/nutrition to reduce exacerbation of the pressure ulcer. The preceptor and personal support worker agree. Explanation: Each healthcare professional is responsible for communicating clearly as well as clarifying discussions or a written order or care plan when it is unclear. |
“Develop trusting relationships with clients/families and other team members” (p. 16). | Example: A doctor writes down an order for pain medication for a client at an inpatient unit. The doctor knows that the nurse is trained to carry out the order. The doctor engages in a discussion with the nurse as follows. Physician: “I wrote an order for Tylenol III, that should help, any questions?” Nurse: “No, that sounds good. I will re-assess their pain after administration and will report any adverse effects of this medication.” Physician: “Great, thanks so much.” Explanation: Trust among the healthcare team (including clients/families) is integral to communication. Part of building trust begins with your interactions with each other. It is important to engage with others in respectful ways and provide time for discussion. Additionally, it is important to be honest in your communication. You should aim to be knowledgeable on the topic and if you are not, open up the discussion in a way that addresses this and allows for a learning opportunity. |
“Effectively use information and communication technology to improve interprofessional client/community-centred care” (p. 16). | Example: The personal support worker routinely documents the amount of food that each client eats at each meal. The personal support worker understands that the healthcare team (dietitian, nurse, physician) will review this information regularly to update client care plans. The updated client care plans are easily accessible within each client’s electronic chart. Explanation: Information and communication technology involving telephone, computers, and software programs can facilitate communication. You will commonly use computer-based documentation systems to document your assessments and plans of care. It is vital that you document clearly and follow the College of Nurses of Ontario (2019) Documentation Standard of Practice. |
Consistent execution of successful communication requires attentive listening skills, administrative support, and collective commitment (Lyndon et al., 2011). Other principles of interprofessional communication include:
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=123#h5p-29
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=123#h5p-30
42
There are several factors that can influence interprofessional communication in positive or negative ways – and can therefore have positive or negative effects on healthcare professionals and client outcomes.
The factors affecting interprofessional communication can be divided into three main categories: those related to the physical environment, those related to the context, and those related to communication styles of the people involved. See Figure 3.4.
Figure 3.4: Factors affecting interprofessional communication
You should consider these factors and how you can modify your communication patterns to engage in effective interprofessional communication.
Table 3.3 presents examples of ineffective interprofessional communication and strategies to manage each one.
Table 3.3: Ineffective communication
*HCP = healthcare professional
Example | Effects | How to manage this type of communication |
Disrespectful communication HCP #1: “It’s 11 am already!” [shakes head in disapproval] “Goodness gracious, you haven’t got her out of bed yet?! What’s wrong with you?” | Demoralizes and demeans another person. Although there may be a reason why the client was not helped out of bed, the healthcare professional may feel disempowered and not share the information. | HCP #2 could respond by saying: “It is probably better for you to inquire about the reasons that I have not got the client out of bed. Your communication is disrespectful and disregards what is going on with Mrs. Hart. Would you like to know what is going on?” Alternatively, HCP #1, who was initially disrespectful, could have engaged in discussion that is guided by inquiry instead of blame, and said: “I noticed Mrs. Hart is not out of bed yet. How can I help?” |
Example | Effects | How to manage this type of communication |
Failure to communicate concern. HCP #1: “The client’s BP is 140/88” HCP #2: “Okay.” | The first healthcare professional stated a finding, but did not indicate or emphasize their concern. Thus, the second healthcare professional did not recognize the need to be concerned or engage in a dialogue. Failure to communicate one’s concern can have a negative effect on patient outcomes. | When communicating, it is important to explicate and emphasize when you have concerns and make sure that the individual that you are discussing it with recognizes the importance of what you are saying. For example, the conversation could be modified such that the concern is acknowledged, and they engage in a discussion about the plan of care: HCP #1: “The client’s BP is 140/88. This is out of the ordinary for this client, their baseline BP is 100/60. I have a serious concern about the high BP and I think we should intervene.” HCP #2: “That is quite a jump. Is the client’s pain well-controlled?” |
Example | Effects | How to manage this type of communication |
Failure to communicate rationale for an action or decision. HCP #1: “Let’s try putting the client in prone position.” HCP #2: “You want us to roll the client onto their abdomen.” HCP #1: “Yes.” HCP #2: “I think that will be difficult.” | The communication is not dialogical because of the failure to communicate a rationale for an action or decision by either of these professionals. As a result, neither professional understands the perspective of the other. | When communicating, it is important to provide rationale for your actions and decisions. For example, the conversation could be modified so that a person’s rationale is clearly identified, as such: HCP #1: “Let’s try putting the client in prone position. Some recent research has suggested that this can improve respiratory function when a client has severe respiratory distress that is not responding to other interventions.” HCP #2: “I am concerned about rolling the client onto their abdomen with all of the tubes and wires. Do you have a suggestion?” HCP #1: “If you are open to it, I can grab one more person and we can do it as a team. What do you think?” |
Example | Effects | How to manage this type of communication |
Unclear/incomplete communication or miscommunication. HCP #1: “Can you help Ms. Di Lallo with her breakfast?” HCP#2: “Yes” HCP#1: “She’s at table 1.” HCP#2: [walks over to the client], “Hi Ms. Di Lallo, are you ready for your breakfast?” Client: “Yes, can you please pass me my coffee?” HCP#2: [passes Ms. Di Lallo her coffee]. HCP#3: “Oh, hold on! Ms. Di Lallo, we need to thicken your coffee first.” | This unclear communication about the client’s diet led to a near miss. Unclear, incomplete, or miscommunication can result in errors related to client care and can have serious consequences for their health. | When communicating, it is important to include all pertinent information to provide safe, effective care. All healthcare professionals need to clarify any communication shared. For example, the conversation could be modified by ensuring communicating all required information: HCP#1: “Can you help Ms. Di Lallo with her breakfast?” HCP#2: “Yes” HCP#1: “Great, she’s at table 1. Ms. Di Lallo has dysphagia, so you need to make sure all her fluids are thickened and follow the dysphagia diet protocol. The thickener should be on her tray. Do you have any questions?” HCP#1: “No, I’m aware of the dysphagia diet protocol and will monitor Ms. Di Lallo during her meal.” |
Example | Effects | How to manage this type of communication |
Ineffective conflict resolution on a plan of care. HCP#1: “Mr. Pink said he does not feel he is ready to be discharged and I agree.” HCP#2: “I think I’m able to determine when Mr. Pink can be discharged considering I’ve been working with him for 6 months and you just met him last week.” HCP#1: “I think we need to talk to the whole team.” | The communication is ineffective because the HCPs disagree about the plan of care for the client. They are not focusing on the context of the interprofessional communication and/or explaining their reasoning based on the client’s needs. They are focusing on their own opinions instead of using a client-centred perspective and evidence-informed approach. | In the case of a disagreement, HCPs need to effectively explain their reasons in the context of client-centred care and evidence-informed approaches. It’s always important to use effective conflict resolution strategies. For example, the conversation could be modified as: HCP#1: “Mr. Pink said he does not feel he is ready to be discharged. I agree with him because he has no support system in place to help him with his activities of daily living at home.” HCP#2: “I believe he is physically and mentally ready to go home, but you bring up a good point. Let’s put together a plan for home care.” HCP#1: “Great.” |
Now, you have learned about the factors that positively and negatively influence interprofessional communication. Inevitably, despite healthcare professionals’ best intentions, conflict is common in interprofessional contexts. Let’s examine this next!
43
Conflict can be defined as a state of serious opposition between two or more perspectives that influences thinking and actions. For example, people may disagree because they have different perspectives. However, varying perspectives alone do not lead to conflict: conflict emerges when one individual’s behaviours impede another individual’s interests or goals, resulting in negative emotions such as fear, anger, and frustration (Barki & Hartwick, 2004, as cited in RNAO, 2012).
Different perspectives will inevitably arise in any context, whether it is at work, with friends, or with colleagues. In an interprofessional environment, different perspectives will occur even when communication is relatively good. For example, healthcare professionals may have different disciplinary perspectives that inform their understanding of a situation, and may have different priorities in terms of client care. Communication can become problematic when these perspectives and priorities contradict another. Conflict is also more likely if interprofessional communication is sub-optimal and ineffective. Other factors that may contribute to conflict include lack of respect for others’ perspective, and differences in values, age, gender, education, ethnicity and culture, as well as elements related to professional roles such as responsibilities, power, and scope of practice (RNAO, 2012).
As shown in Figure 3.5, you can consider several strategies to prevent or manage conflict including:
Figure 3.5: Conflict management strategies .
First, use a client-centred approach. This ensures the focus is on the client as a whole person and that the patient is cared for in ways that respect their “autonomy, voice, self-determination, and participation” in their own care (Registered Nurses Association of Ontario, 2006).
Second, use an evidence-informed approach. This will help you critically engage in discussions that are informed by the evidence, rather than personal preference.
Third, it is essential that you be open to hearing, respectfully discussing, and reflecting on the perspectives of all team members (Lyndon et al., 2011). In addition to sharing your perspective, share the rationale for it. Along with a client-centred and evidence-informed approach, this kind of effective dialogue will benefit the person who is the focus of care and decisions: the client.
Points of Consideration
Interprofessional communication can be optimized using a client-centred perspective and an evidence-informed approach. It should be guided by discussions that are centred on the client’s wellbeing and incorporate the best possible evidence for each client.
Preventing and managing interprofessional conflict involves responsibility at both individual and systemic levels. The interpersonal nature of conflict is important, but contextual and organizational factors can also contribute. In the context of nursing, interprofessional team members are often working in environments where they are dealing with feelings such as frustration, burnout, dissatisfaction, and a sense of being undervalued. This kind of environment requires a high level of acuity and can be very emotionally draining.
It is imperative to consider whether healthcare organizations and systems are supporting collaboration and conflict resolution, or contributing to negative emotions (RNAO, 2012). For example, are processes and systems set up for easy communication? Do teams work together or are there divisions and hierarchies? Is there shared decision-making and accountability, or a culture of blame, disrespect, and fear of reprisal? Are certain health professionals particularly overworked? To prevent and reduce interprofessional conflict, the RNAO (2012) has developed specific recommendations for organizations to consider related to organizational structures and climate, leadership support, staffing practices, communication practices, and professional components.
The next section explores what can happen if conflicts are left unresolved and escalate to harassment and bullying.
44
Effective intraprofessional (within a discipline) and interprofessional (across disciplines) communication and interactions are essential to effective work environments and quality and safety in healthcare. Civility is a key component of effective communication and interactions, and is particularly important because of the stressful and complex nature of healthcare environments and decision making.
Civility involves treating others (e.g., healthcare team members) with respect, listening to their perspective, considering their feelings within an encounter, and respecting differences, but also working to seek common ground when needed. It is essential to emphasize that civility involves engaging in authentic, respectful, and inclusive ways with others; civility fosters a feeling of belonging and community even when there is conflict or differences in perspectives (Clark et al., 2022).
Incivility is a serious issue in teamwork (in both intraprofessional and interprofessional environments). Incivility within communication encounters or interactions involves the covert (subtle) or overt disrespect of another person. Examples include discourtesy, eye rolling, gossiping, rude comments, name calling, complaining, and physical actions including violence – all of these behaviours that can cause emotional and physical harm to a person. Conflict management strategies and communication training are known to assist nurses to deter and address uncivil behaviours as well as foster clarity and trust.
Bullying and harassment are often referred to as types of incivility addressed to a specific person. Although these terms are similar, harassment specifically is a type of discrimination based on factors such as religion, race, age, sex, and disability (Canadian Human Rights Commission, n.d.). Bullying and harassment are typically repetitive behaviours (happen more than once) and harm or humiliate another person. However, they can also include serious one-time incidents of unwanted verbal and/or physical behaviour (Canadian Human Rights Commission, n.d.).
These behaviours usually occur in the context of a real or perceived power imbalance. For example, the person who is bullying often thinks they have more power (e.g., more seniority, authority, specialized title/role, more education). This type of incivility may also occur between nurses as forms of horizontal violence, which is lateral violence within a group.
Many forms of harassment and bullying can occur within the nursing profession (intraprofessional) and across various healthcare professionals (interprofessional). They may be physical such as unwelcome touching of your body or the attire you wear. More often, they take the form of non-verbal and verbal behaviours. This includes demeaning, humiliating, and belittling language, hurtful teasing/jokes, name-calling, slurs, insults, and criticism as opposed to critique. Non-verbal behaviours specifically can include eye-rolling and other facial and bodily expressions. Other bullying and harassing behaviours include ostracism and purposefully ignoring someone and not helping colleagues or continually assigning someone workloads that are considered difficult and problematic.
Keep in mind that intraprofessional or interprofessional conflict does not constitute incivility or harassment. You will have conflict in the workplace where you have strong opposing points of view. Additionally, your supervisor or a peer may even provide feedback or constructive criticism in a supportive manner – this also does not constitute incivility or harassment. There may be uncivil behaviour in the workplace that also does not constitute harassment or bullying, but still should be addressed (Government of Canada, 2015).
You may not readily recognize that you are being bullied or harassed, and not everyone who bullies or harasses is aware of behaviour. Sometimes these behaviours arise because of interprofessional conflict, but they can also be caused by personal issues. For example, healthcare team members could have stress at home, financial concerns, or anger management issues. All of these factors can affect how they engage with others in all settings, including the healthcare environment – and the stresses associated with the healthcare environment can also be contributing risk factors.
Whatever the reason, you have the right to a workplace that is free from any form of incivility including bullying and harassment. See Figure 3.6.

Figure 3.6: Workplace free from harassment
Professional nursing associations have been instrumental in addressing and managing bullying and harassment in the workplace. It is important for all nurses to attend to this form of violence in the workplace and take a leadership role in order to make change. Nursing has a legacy as an oppressed group because of its history as a subordinated profession (i.e., being considered subservient to the medical community) and because of socio-cultural structures like nursing being deemed gendered work. Oppressed group behavior can lead to horizontal violence, when parties in the same group lash out or exhibit violence toward each other in response to external dominant power. In such cases, members of an oppressed group feel subjugated and powerless against a dominant group and essentially take it out on each other. It is important to be aware of this dynamic as we work toward creating workplaces that are free from and intolerant to violence.
Why is it important to understand incivility, violence, harassment, and bullying?
Violence, harassment, and bullying are identified as occupational health and safety hazards that are underreported and often unrecognized (Becher & Visovsky, 2012).
As a nursing student, you need to be aware of what incivility, harassment, and bullying are and how to deal with them. These behaviours are not always conscious choices, so self-reflection and awareness are important first steps toward eliminating this type of incivility and violence in the workplace. Being the victim of bullying can have traumatic effects on self-esteem, mental health, and confidence in the workplace. Additionally, systemic bullying within an interprofessional team setting can affect staff morale, job performance, team functioning, and importantly, client care.
What should you do if you observe incivility, or someone being harassed?
First, if you observe incivility, step in and support the person on the receiving end.
Second, if you feel comfortable and safe, have a discussion with the person who is demonstrating the uncivil behaviour. Avoid participating in confrontational dialogue. Engage in an inquisitive discussion to better understand why it is occurring, and, if the person understands what they are doing and its impact on the other person. For example, you might say to them, I noticed that you have repeatedly rolled your eyes and interrupted X when they were sharing their perspective. Were you aware of that behaviour?
Third, if the incivility or harassment continues, report and document the incidents to your manager and the human resources department. If it is your manager who is creating the uncivil environment or doing the harassing, human resources should be your main point of contact.
Points of Consideration
“I am a nursing student. What should I do if I believe I am experiencing incivility in the learning environment or feel that I am being harassed or bullied in my clinical placement or in school?”
First, recognize this is not your fault and you do not deserve this. You have the right to a civil learning environment free of incivility, violence, harassment, and bullying. You deserve to be respected and supported in your learning.
Consider how to respond using conflict resolution strategies: https://pressbooks.library.ryerson.ca/communicationnursing/chapter/professional-communication-in-conflict-resolution/ Although it may not seem like it, the person who may be creating the incivility in the learning environment or doing the bullying or harassment might not realize they are doing it and they may not realize the impact of their actions. It is always best to speak with the person if you can do so. Have a private conversation and share your perspective and how you are being affected, but do so in a non-confrontational manner.
If at first, you feel too intimidated to do so, consider speaking with an instructor or a trusted individual within your school or university so that they can support you, brainstorm with you about how to approach the situation, and if needed, provide appropriate resources. In some cases, your support person may advise you to contact a senior leader in the school or possibly the Office of Discrimination and Harassment Prevention Services, or the Office of Sexual Violence Support and Education (these are services at Ryerson University, but all institutions have similar resources).
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=129#h5p-31
45
There are numerous resources to facilitate interprofessional collaboration and teams, including interprofessional communication.
Ideally, all healthcare professionals including nurses would speak up for the sake of clients, clearly state what they think is happening in a specific situation, and explain what and why they think certain actions should be taken (Lyndon et al., 2011). However, some healthcare professionals may struggle to voice their concerns and their perspectives, particularly if they feel less empowered or marginalized by another healthcare professional. One objective of interprofessional communication tools is to provide structure and clarity to convey succinct, comprehensive, and relevant information to another healthcare professional to improve client care.
Several standardized tools have been developed to facilitate interprofessional communication (Canadian Medical Protective Association, 2011) and prevent and manage harassment, errors in the workplace, and miscommunication. The SBAR tool, and its variations including ISBAR, is one common communication tool that can facilitate effective verbal communication when communicating with another healthcare professional about a client or during handover. It provides a framework so that communication is focused, concise, and complete.
ISBAR, detailed in Figure 3.7, is an acronym for Introduction, Situation, Background, Assessment, Recommendation. It was first introduced by the military in the United States to facilitate communication (NHS Improvement, n.d.) and has since been taken up in the healthcare arena to enhance client safety by facilitating communication among healthcare professionals and ensure the most important information is included (NHS improvement, n.d.; Spooner et al., 2016).
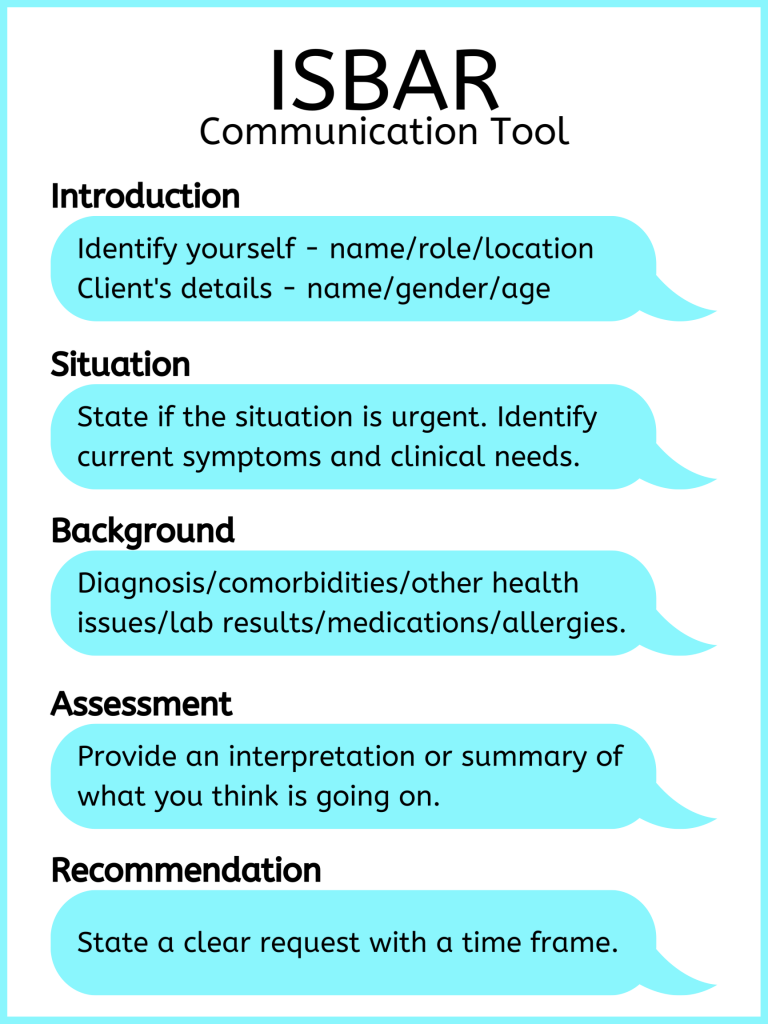
Figure 3.7: ISBAR
Using the ISBAR effectively takes practice. Check out Film Clip 3.1 about ISBAR [3:08].
Film Clip 3.1: ISBAR
Research suggests that nurses do not comprehensively use elements of ISBAR, and the sections on assessment and recommendation are consistently neglected (Spooner et al., 2016). It is important to reflect on how you communicate and how you can improve through comprehensive use of tools. See Table 3.4 for an example of effective use of the ISBAR to guide communication.
Table 3.4: Example of ISBAR Use
I – Introduction
| “Hello, I am calling about Zina Mills, a 45-year-old female client on 3C. I am Sandu Martique, a registered nurse on the unit.” |
S – Situation
| “The client is experiencing shortness of breath with a productive cough, and green mucous times three days. Currently, she has moderate crackles throughout the left lobe. 02 sat is 90%, respiratory rate is 26, temp is 38.3, pulse 98, blood pressure 134/88, and she is on 4 litres oxygen via nasal prongs.” |
B – Background
| “The client has been in this facility for 4 days following hip surgery. Her incisions show no signs of infection. However, her mobility has been limited due to moderate dementia. She has a history of hypertension, no previous lung disease, and is a non-smoker.” |
A – Assessment
| “Based on my assessment, her symptoms may be associated with pneumonia.” |
R – Recommendation
| “Would you like a chest x-ray done? And when do you have time to see the client?” |
Points of Consideration
Think about what you want to say and how you want to say it before you say it. Organize your thoughts first.
An interactive H5P element has been excluded from this version of the text. You can view it online here:
https://pressbooks.library.ryerson.ca/communicationnursing/?p=131#h5p-35
46
In a workplace setting, you are responsible for your own communication, actions, and behaviours. You should begin by engaging in self-reflection. Start by thinking about your personal values concerning communication. What factors do you believe are important in shaping how you communicate effectively? How do you speak with others? What bothers you or empowers you within a communication encounter? What are your strengths when communicating with another person? What are some areas for improvement in your communication? Consider how your strengths and barriers may influence a communication encounter. For example, how do barriers influence your capacity to engage in communication and your capacity to deliver and receive a message?
Some of your communication barriers may be very personal and may have developed when you were a child. Reflect on the following questions:
Next, reflect on the professional values of communication and nursing that you strive to achieve. You may consider these in the context of the nursing role and what is expected of you as a nurse. For example, competencies for entry-to-practice involve roles associated with being a communicator, an advocate, a collaborator, and a leader (College of Nurses of Ontario [CNO], 2018). Each of these roles will require you to communicate and use a variety of strategies, including conflict resolution, to “create and maintain professional relationships” (CNO, 2018, p. 6).
Some of your communication barriers may be related to your professional capacity. Reflect on the following points:
47
Key Takeaways
48
Becher, J., & Visovsky, C. (2012). Horizontal violence in nursing. Medsurg Nursing, 21(4), 210-213.
Canadian Human Rights Commission. (n.d.). What is harassment? https://www.chrc-ccdp.gc.ca/en/about-human-rights/what-harassment
Canadian Interprofessional Health Collaborative. (2010). A national interprofessional competency framework. https://phabc.org/wp-content/uploads/2015/07/CIHC-National-Interprofessional-Competency-Framework.pdf
Canadian Medical Protective Association. (2011). Strengthening inter-professional communication. https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2011/strengthening-inter-professional-communication#structured_communication_tools
Canadian Nurses Association. (n.d.a). Position statement – Interprofessional collaboration.
Canadian Nurses Association. (n.d.b). Joint position statement – Workplace violence and bullying. http://cna-aiic.ca/~/media/cna/page-content/pdf-en/workplace-violence-and-bullying_joint-position-statement.pdf
Clark, C., Gorton, K., & Bentley, A. (2022). Nursing Outlook (in press). https://doi.org/10.1016/j.outlook.2021.11.001
College of Nurses of Ontario. (2018). Entry-to-practice competencies for registered nurses. https://www.cno.org/globalassets/docs/reg/41037-entry-to-practice-competencies-2020.pdf
Government of Canada (2015). Is it harassment? A tool to guide employees. https://www.canada.ca/en/government/publicservice/wellness-inclusion-diversity-public-service/harassment-violence/harassment-tool-employees.html
Registered Nurses Association of Ontario. (2006). Client centred care. https://rnao.ca/sites/rnao-ca/files/Client_Centred_Care.pdf
Lyndon, A., Zlatnik, M., Wachter, R. (2011). Effective physician-nurse communication: A patient safety essential for labor & delivery. American Journal of Obstetrics & Gynecology, 205(2), 91-96. doi: 10.1016/j.ajog.2011.04.021
NHS Improvement. (n.d.). SBAR communication tool – situation, background, assessment, recommendation. Retrieved from: https://improvement.nhs.uk/documents/2162/sbar-communication-tool.pdf
Spooner, A., Aitken, L., Corley, A., Fraser, J., & Chaboyer, W. (2016). Nursing team leader handover in the intensive care unit contains diverse and inconsistent content: An observational study. International Journal of Nursing Studies, 61, 165-172.
1
A type of question that invites the client to share descriptive answers, open up about their experience, and let them answer in a way that is most relevant or comfortable from their perspective.
Care partners are family and friends who are involved in helping to care for the client.
A direct question that is asked when you are seeking precise information.
A direct question that is asked when you are seeking precise information.
Fair opportunity to reach one’s fullest health potential.
testing
A type of question that invites the client to share descriptive answers, open up about their experience, and let them answer in a way that is most relevant or comfortable from their perspective.
Assumes each person is a relational being who is influenced by those around them, their communities, and social and cultural processes.
Assumes trauma, does not require disclosure, and promotes client safety, control, and choice.
A statement that refers to how someone behaves and acts and encompasses both verbal and non-verbal communication.