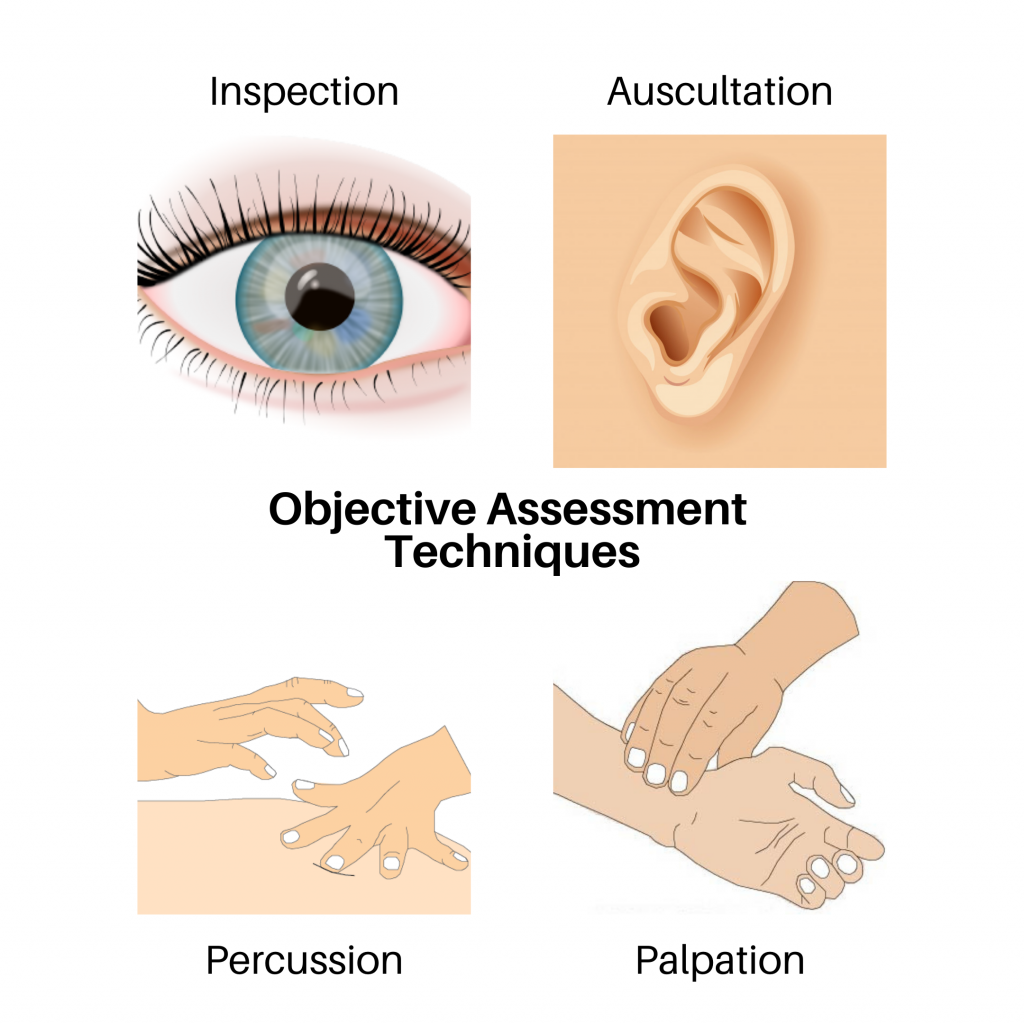
This open access textbook is an introductory resource to guide best practices of objective assessment techniques related to inspection, palpation, percussion, and auscultation (IPPA). Its intended audience is students in health-related post-secondary programs such as nursing.
This book is best viewed via the online, Pressbooks format so that you can view the videos and participate in the interactive components. However, a pdf format is also available.
About the Authors
Jennifer Lapum, PhD, MN, BScN, RN, Professor, Daphne Cockwell School of Nursing, Ryerson University, Toronto, ON, Canada
Michelle Hughes, MEd, BScN, RN, Professor, Professor, School of Community and Health Studies, Centennial College, Toronto, ON, Canada
Oona St-Amant, PhD, MN, BScN, RN, Assistant Professor, Daphne Cockwell School of Nursing, Ryerson University, Toronto, ON, Canada
Wendy Garcia, MN, BScN, RN, Instructor, Ryerson University, Faculty of Community Services, Daphne Cockwell School of Nursing, Toronto, ON, Canada
Margaret Verkuyl, MN, NP:PHC, Professor, Centennial College, School of Community and Health Studies, Toronto, ON, Canada
Paul Petrie, RN, BScN, MScN, Professor, George Brown College, Sally Horsfall Eaton School of Nursing, Toronto, ON, Canada
Frances Dimaranan, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Mahidhar Pemasani, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Nada Savicevic, MA Interactive Design, MArch, BSc (Eng), Instructional Designer, Office of e-Learning, Ryerson University, Toronto, ON, Canada
Contact person
Dr. Jennifer L. Lapum
jlapum@ryerson.ca
415-979-5000 ex. 556316
350 Victoria St., Toronto, ON, M5B 2K3
@7024thpatient
Note to Educators Using this Resource
We encourage you to use this resource and would love to hear if you have integrated some or all of it into your curriculum. If you are using it in your course, please consider notifying Dr. Lapum and include the course/program and the number of students.
Funding
This project was supported by a Ryerson University Library OER grant.
Student Advisory Committee
Agata Arent, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Lauren Baljeu, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Meera Chawda, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Nicolas D’Ambrosi, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Veronica Fedal, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Fonda Tran, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Jacqueline Zampese, BScN student, Ryerson, Centennial, George Brown Collaborative Nursing Degree Program, Ryerson University, Toronto, ON, Canada
Acknowledgments
Arina Bogdan, BScN, RN, Ryerson University (artist of the front cover artwork)
Adam Chaboryk, IT Accessibility Specialist, Digital Media Projects, Ryerson University
Linn Clark, Editor, Toronto, Ontario, Canada
Ann Ludbrook, Copyright and Scholarly Engagement Librarian, Ryerson University
Jeevan Marway, BScN, RN, MN, Trillium Health Partners.
Nada Savicevic, Interactive Design, Educational Developer, Centre for Excellence in Learning and Teaching, Ryerson University, Toronto, Ontario, Canada
Sally Wilson, Web Services Librarian, Ryerson University
Contributors – Voices of Experience
Yvette Dalrymple, RN(EC), NP Paediatric, CPHON
Vikky Leung, MN, BScN, BSc, RN, Emergency Department, The Hospital for Sick Children, Nursing Clinical Instructor, Centennial College
Andrea McGowan, BScN, RN, CNE, Island Health – Vancouver Island Health Authority
Cheryl Tai, NP-PHC, MN, Contract Lecturer, Daphne Cockwell School of Nursing, Ryerson University
Customization
This textbook is licensed under a Creative Commons Attribution 4.0 International (CC-BY NC) license except where otherwise noted, which means that you are free to:
SHARE – copy and redistribute the material in any medium or format
ADAPT – remix, transform, and build upon the material for any purpose, even commercially.
The licensor cannot revoke these freedoms as long as you follow the license terms.
UNDER THE FOLLOWING TERMS:
Attribution: You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
No additional restrictions: You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
Notice: You do not have to comply with the license for elements of the material in the public domain or where your use is permitted by an applicable exception or limitation.
No warranties are given. The license may not give you all of the permissions necessary for your intended use. For example, other rights such as publicity, privacy, or moral rights may limit how you use the material.
The following attribution statement should be included when using parts of this OER:
© 2020 Ryerson University. Licensed under a Creative Commons Attribution 4.0 International License (CC-BY NC). Communication for the Nursing Professional (1st Canadian edition) by Jennifer L. Lapum, Michelle Hughes, Oona St-Amant, Wendy Garcia, Margaret Verkuyl, Paul Petrie, Frances Dimaranan, Mahidar Pemasani, Nada Savicevic. Download this book for free at: X