
Chapter 11 – Cardiovascular System Assessment
Auscultation of the Cardiac Valves
Auscultation provides information about the functioning of the cardiac valves, for example whether they are opening and closing appropriately and the quality of blood flow through the valves. Cardiac valves include the atrioventricular valves (AV) (tricuspid and mitral) and the semilunar valves (SL) (aortic and pulmonic). Remember, auscultate them at the location that corresponds with the flow of blood out of the valve, not at their anatomic location.
Biological background of heart sounds
You need to know what you are listening for when auscultating the valves. First, you are listening for heart sounds (“lub dub”). As described above, these sounds are related to the closing of the heart valves and referred to as S1 (lub) and S2 (dub). In a healthy heart with no valvular pathology, the opening of these valves is silent.
- S1 is the closing of the AV valves including the tricuspid valve and the mitral valve. Although the mitral valve closure occurs immediately prior to the tricuspid valve closure because of the route of electrical charges in the heart (i.e., myocardial depolarization), the closing of these valves are generally heard at the same time in the healthy heart – lub.
- S2 is the closing of the SL valves including the aortic valve and pulmonic valve. Although the aortic valve closure occurs immediately prior to the pulmonic valve closure because of the route of electrical charges in the heart, the closing of these valves are generally heard at the same time in the healthy heart – dub.
Recall what you learned in biology:
- S1 involves the closing of the AV valves, so it is considered the beginning of systole (contraction of the ventricles ejecting blood into the pulmonary artery and the aorta).
- When the AV valves close, all four cardiac valves remain closed momentarily (it’s called isovolumetric contraction) and then the semilunar valves (aortic and pulmonic) open while the ventricles contract.
- Then, the semilunar valves close (S2); this is considered the end of systole and the beginning of diastole (relaxation of the ventricles filling with blood)
- When the semilunar valves close, all four cardiac valves are closed momentarily (this is called isovolumetric relaxation) and then the AV valves open and the ventricles fill with blood (i.e., diastole).
Auscultating cardiac valves
The steps involved in auscultation of the cardiac valves are (see Video 10):
1. Keep the client in a supine position and use draping.
- You can do this assessment with the client in a sitting position, but it is generally easier to do in a supine position because you can drape the client without struggling to hold the drape in place. Also, you might have to ask a client who is sitting to reposition their breasts to auscultate the valves; this is easier in a supine position as larger breasts will typically shift laterally in a supine position.
- NOTE: if you have specific cardiac concerns, you should also listen for murmurs in the left lateral position and in the sitting position with the client leaning forward slightly. This positioning can help you hear any murmurs that might be present.
2. Cleanse the stethoscope.
3. Follow the pattern in Figure 8 to auscultate the cardiac valves.
- Particularly when you have concerns, some practitioners will move their stethoscope around several locations at each site.
- Remember, it is important to physically landmark the location of the valves immediately before you auscultate them.
-
- Landmarking for these valves is important. For a reminder about landmarking, go back to The Heart page to watch the video.
4. Auscultate all four valves with the bell, and then begin again and auscultate all four valves with the diaphragm.
- Heart sounds are typically classified as low-pitched, but you should use both the bell and diaphragm to distinguish sounds because some may be better heard with the diaphragm versus the bell. For example, S1 is lower in pitch than S2 and some abnormal heart sounds are higher in pitch.
- At each location, listen as long as you need to complete the assessment, but for at least two to three full cardiac cycles (including systole and diastole). You may need to listen longer if you hear abnormal sounds.
- S1 and S2 – (lub dub) Are they clear and distinct sounds? Or do you hear split sounds associated with S1 and S2? This can occur when the tricuspid and mitral valve do not close at the same time or the aortic and pulmonic do not close at the same time.
- Murmurs are a whooshing sound associated with turbulent blood flow that can occur when a valve is not opening and closing appropriately. See Audio 4.2 to hear what a murmur sounds like. When a valve is not working properly, this can lead to of blood. Sometimes a murmur is caused by heightened blood flow such as during pregnancy or exercise. Assess whether murmurs are present or absent; if you hear a murmur, the main characteristics to be evaluated are:
- Timing with the cardiac phase. Is it associated with S1 or S2?
- Grading of the loudness of the sound (see Table 2). Murmurs that are grade 4 and above are associated with a palpable thrill.
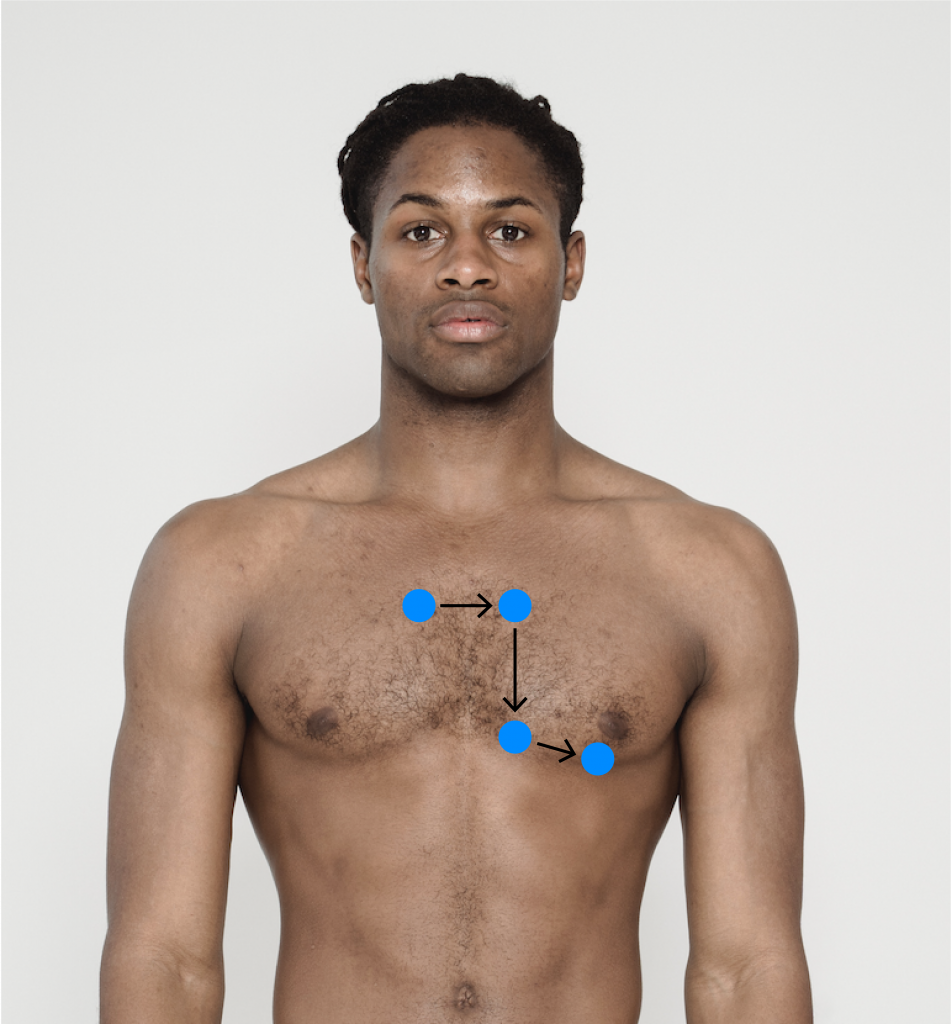
Figure 8: Pattern for auscultation of cardiac valves
5. Note the findings
- Normal findings might be documented as: “Clear S1 and S2, no split sounds, no murmurs.”
- Abnormal findings might be documented as: “Clear S2, no split sounds, grade II murmur heard best on S1, at the apex.” (This is just one example of an abnormal finding that could be associated with .)
Audio 2: Normal S1/S2 sounds.
Audio 3: Murmur.
(Attribution statement: taken from https://wtcs.pressbooks.pub/nursingskills/chapter/9-3-cardiovascular-assessment/)
Table 2: Levine’s murmur scaled (adapted from Silverman & Wooley, 2008).
| Grade 1 | Faint/difficult to hear (not heard right away) |
|---|---|
| Grade 2 | A faint murmur heard immediately |
| Grade 3 | Moderately loud murmur |
| Grade 4 | Loud murmur |
| Grade 5 | Very loud murmur. Can be heard if only the edge of the stethoscope is in contact with the skin. |
| Grade 6 | Loudest possible murmur. The murmur can be heard with the stethoscope just removed from the chest and not touching the skin. |
See Video 11 for an in-depth understanding of heart sounds: the main point is that heart sounds can change based on cardiac pathologies. Heart Sounds | Complete Cardiac Sounds with Audio | Heart Sounds Made Easy.
Video 10: Auscultation of cardiac valves.
Video 11: Heart sounds.
Knowledge Bites – Pathophysiology
The cardiac valves may be associated with many issues, most commonly regurgitation/prolapse and stenosis. Regurgitation is leaking or backflow of blood through the valve; this is sometimes caused by prolapse in which the valve does not close completely. Stenosis involves narrowing of the valve, which limits/restricts blood flow through the valve.
Activity: Check Your Understanding
Reference
Silverman, M., & Wooley, C. (2008). Samuel A. Levine and the history of grading systolic murmurs. The American Journal of Cardiology, 102(8), 1107-1110. https://doi.org/10.1016/j.amjcard.2008.06.027
refers to blood leaking backwards through the valve.
refers to when the valve does not fully close and blood flows backwards.
