Introduction
Theoretical Perspectives and Competencies
Dr. Sue Bookey-Bassett; Dr. Sherry Espin; and Sukhanjit Kaur
Theoretical Perspectives and Competencies
This work is influenced by several theoretical perspectives and frameworks that support the need for education about integrated interprofessional stroke care in a community setting. Please refer to Appendix A for detailed information on the theoretical perspectives and competencies that were considered. These include:
Integrated Stroke Care
Integrated care brings together components of design and delivery of care that are fragmented, and integrates those parts together to form a whole that optimizes care provision (Goodwin, 2016). Services, providers, and organizations from across care settings and sectors come together to work jointly, complement each other, and act in coordination with each other to ensure a seamless, unified system with continuity (Markle-Reid et al., 2020). During the acute phase of stroke care, patients are admitted to a stroke unit where an interprofessional stroke team assists with initiating early rehabilitation for patients (Toronto Stroke Networks, 2023). This team may consist of physicians, nurses, occupational therapists, pharmacists, clinical nutritionists, social workers, physiotherapists, and speech-language pathologists (Toronto Stroke Networks, 2023).
Once patients are ready to transition out of acute care hospital settings, evidence supports the need for ongoing integrated interprofessional stroke-specific care in the community. A 2023 randomized controlled trial conducted by Markle-Reid et al. in Canada found that patients who received integrated interprofessional care in the community setting for 6 months had significantly greater gains in self-reported physical functioning, stroke self-management, and patient experience.
Stroke Care Transitions
When transitioning patients out of the acute care phase of their journey, there is a need for safe transfer of patient information and care needs to prevent a breakdown in care processes (Registered Nurses Association of Ontario, 2023). This is essential to ensure a seamless integration of care across facilities (acute and community care facilities) and interprofessional teams, as it facilitates coordination within teams (Markle-Reid et al., 2020).
The Heart and Stroke Foundation’s 2019 Canadian Stroke Best Practice Recommendations for Rehabilitation, Recovery and Community Participation
The Canadian stroke best practice recommendations for rehabilitation, recovery, and community participation, provided by the Heart and Stroke Foundation (2019), support the need for and stress the importance of integrated and coordinated care across the healthcare system. This guideline was published with the goal of optimizing stroke care across Canada, reducing variations in how care is received by stroke patients, and closing the gap between research and practice (Heart and Stroke Foundation, 2019).
Kolb’s Experiential Learning
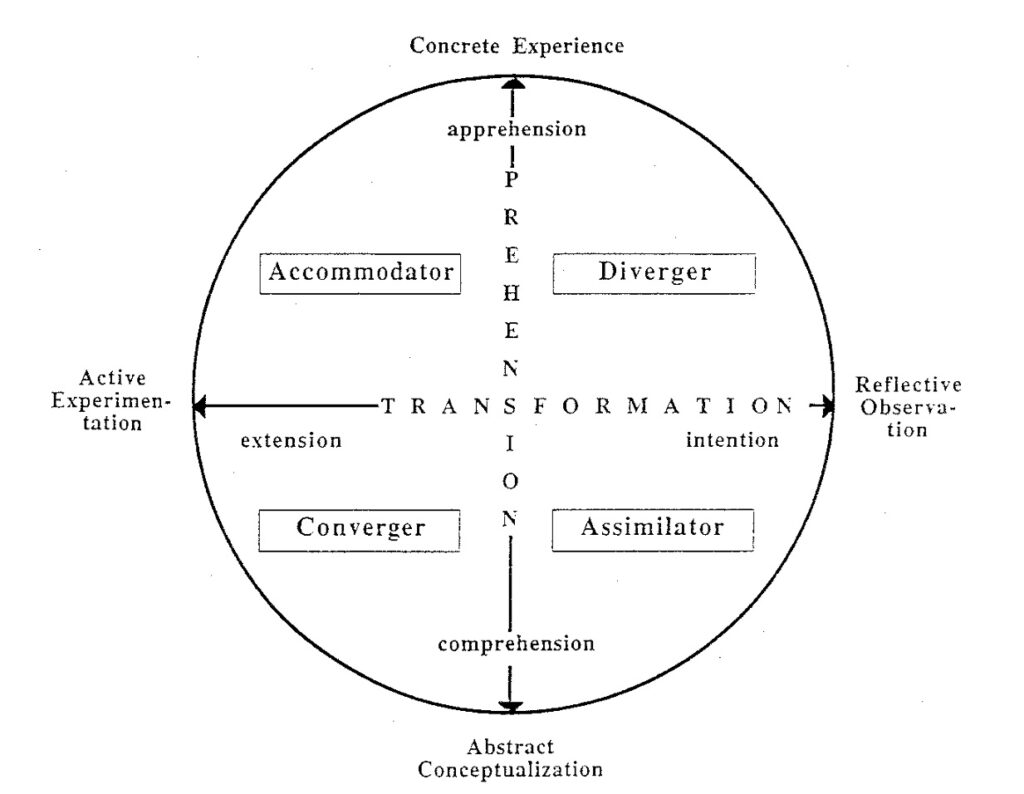
Kolb’s (1984) theory of experiential learning guided the design and delivery of this learning activity. The theory posits that education is experiential and that learning occurs through the reconstruction and critical reflection of experiences (Kreber, 2001). Learners begin by engaging with a concrete experience through direct, sensory, and intuitive interaction (Kreber, 2001). Then, they thoughtfully observe and reflect on their experience, leading to the creation of an abstract conceptualization of it through analytical or symbolic understanding (Kreber, 2001). And finally, they actively experiment with the new information through practical application (Kreber, 2001). These four processes form the four stages of the learning cycle (Kreber, 2001).
Figure 1
Kolb’s (1984) Model of Experiential Learning
The World Health Organization Rehabilitation Competency Framework (2021)
The World Health Organization’s (2021) rehabilitation competency framework provides competencies for all rehabilitation workers in the domains of practice, professionalism, learning and development, management and leadership, and research. This competency framework guides both rehabilitation workers’ approach to practice and their daily practice activities. It addresses important concepts such as patient-centered care, collaboration, effective communication, and working effectively within a team approach to service delivery (World Health Organization, 2021).
Figure 2
Description of the Five Domains of the RCF

Competency Framework for High-Quality Workforce Development in Integrated Care (2024)
This competency framework for high-quality workforce Development in Integrated Care, developed by Barraclough et al. in 2024, guides the development of this project. This framework provides the necessary competencies for the provision of training in integrated care in the following areas:
- Person-centered care
- Interprofessional teamwork and collaborative practice
- Care coordination
- Digital skill and technology
- Health promotion and disease prevention
- Population health approach to care
- Leadership
- Professional and ethical attributes
The Stroke Specific Education Framework by the University of Central Lancashire and the National Health Service in England (2022).
The framework for stroke specific education created by the University of Central Lancashire and the National Health Service of England (2022) outlines the knowledge and skills required of healthcare professionals working with patients with stroke. This framework comprises of 16 elements of care and 4 elements of professional practice. For the purposes of this learning experience, please refer to:
- Element 10: Specialist Rehabilitation
- Element 12: Seamless transfer of care
- Element 13: Long-term care
- Element 14: Review
- Element 15: Participation in community
- Element 16: Return to work
- Element 17: Professional behaviour and values
- Element 19: Education, training, and personal development
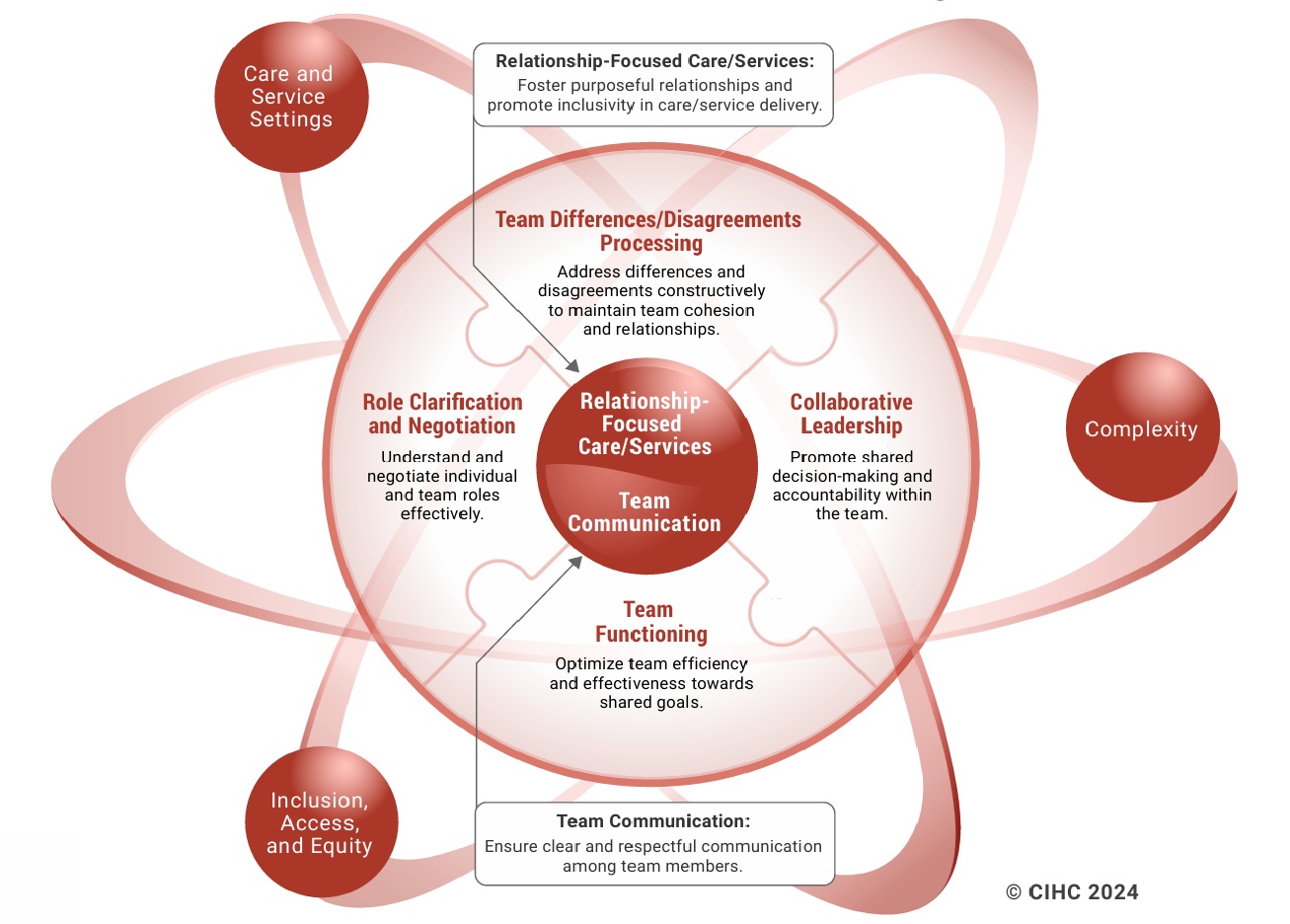
The Canadian Interprofessional Health Collaborative Competency Framework for Advancing Collaboration (2024)
The Canadian Interprofessional Health Collaborative (CIHC) Framework (2024) guides educators, researchers, health administrators, service providers, and persons receiving care in fostering effective collaborative practice. The framework focuses on supporting the application of knowledge, skills, attitudes, and values in real-world environments to guide behaviours that enhance collaboration. The framework has six competency domains which are interdependent.
The overarching goal of this framework is to improve healthcare and human services by promoting collaborative, relationship-focused partnerships for shared decision-making.
Figure 3
Description of the Five Domains of the RCF