
Frontline Service Providers
Chapter 15: Responding to TFGBV as Frontline Service Providers
In this chapter, we want to equip frontline service providers with a trauma‑ and disability‑informed approach to TFGBV, using a survivor centered approach. It centers an applied case, practical frameworks, and ready‑to‑use tools for assessment, documentation, immediate safety, and referral.
Learning Objectives
- Learn foundational principles of GBV responses and survivor-centered care.
- Apply the Ask–Validate–Document–Refer framework in digital abuse disclosures, centering survivors throughout.
- Identify local and organizational referral pathways for survivors of digital abuse.
- Integrate emotional support while preserving survivor autonomy and safety.
Foundational Principles for Safe Responses
In your approaches to client disclosures of TFGBV there are several general considerations that you need to make regarding how to proceed in ways which are empowering to the survivor.
In general, following Gender-Based Violence (GBV) guiding principles (keeping standards of safety, confidentiality, respect, and non-discrimination) and a survivor-centered approach (ensuring that survivors’ experiences and wishes are central and essential to guiding decisions and actions) are vital to best practices.
Gender-Based Violence (GBV) guiding principles are as follows:
- Safety-based approach. Attending to both immediate, short-term, and long-term physical, emotional, mental, and digital risks.
- Confidentiality. Give the survivor control over what is shared and when. Women with disabilities are frequently stripped of autonomy due to societal and structural barriers, and it is essential that service providers do not continue to do this. However, there are some limits to confidentiality, and service providers should inform survivors of this.
- Respect. Respect the choices and dignity of all people who you serve, by including them, respecting their identity and experiences, and approaching with openness.
- Non-discrimination. All actions should be informed with approaches that acknowledge the many parts of a person and survivor. Gender, race, disability, sexual orientation, religious affiliation and any other identifiers should be respected and approached without bias.
To learn more about GBV Principles, you can go to the resource from the UNFPA, which is linked here.
Core parts of a survivor-centered approach to GBV also include:
- Trustworthiness. Be transparent about limits of confidentiality and next steps. Disability and gender-based stigma experienced in many societal spheres can create atmospheres of distrust and fear.
- Collaboration. Aim to co‑create safety plans and referrals with your clients. Nothing should occur without survivors’ consultation and involvement, except in extreme circumstances.
- Empowerment. Support digital autonomy and reduce shame around experiences. You can do this by providing resources around digital literacy and digital safety that are accessible, and facilitating teaching digital safety in ways that support self-sufficiency.
Reflect
- What barriers in your context (healthcare, GBV support, advocacy, disability rights, et cetera) can you foresee in applying these principles?
- How might you plan to overcome or circumvent these barriers?
Using an Ask–Validate–Document–Refer framework
This framework provides a simple, structured way to respond to TFGBV disclosures.
Ask (permission first): Ask about TFGBV.
Ask permission to discuss, and then about the TFGBV. Ask about frequency, content, sender identity, platforms used, whether images were shared, and whether the perpetrator has offline access to locations or contacts.
- Try phrases like: “May I ask some questions about what happened and how it’s affecting you? You can stop at any time.”
Validate: Validate the experience.
- Avoid blame or minimising language; do not pressure immediate reporting unless there is an emergency situation.
- Try phrases like: “That sounds frightening”; or, “You did the right thing telling me.”
Document (with consent): Record evidence.
- Record verbatim statements, dates, times, platforms, and witnesses. Note whether the client consents to evidence collection and sharing. Use the documentation template below.
Refer: Refer to services.
- Offer options that you are able to directly refer them to, such as legal advice, digital forensics, police follow‑up, psychosocial counselling, medical appointments, shelter services, and peer support. Let the survivor choose which referrals to accept and when.
The AVDR framework ensures that responses remain structured, supportive, and aligned with the survivor’s needs.
Developing an AVDR framework requires an organisation or institution has a base of knowledge around locally available facilities and services. If this is not yet in place, we deeply encourage a review of your internal policies and services. For reference, we have compiled a list of resources and services in South Africa, which may be useful to you, which is linked on our Support and Resources Page.
Communication with Clients Around TFGBV
Clear, respectful language supports safety and trust during difficult conversations. Example of possible scripts to use through the service delivery and reporting or response process include:
- “I’d like to write down what you’ve shared so we can support you appropriately. Is that okay?”
- “If there is an immediate risk to your safety, I may need to involve others. I will tell you before I do that.”
- “I can connect you with legal support, a forensic specialist, or a counsellor. What would you prefer at this stage?”
Incident Report Flow Charts
An incident‑report flow chart helps frontline workers know exactly what to do when TFGBV is suspected or disclosed, and to progress through the AVDR stages. Because digital abuse can escalate quickly and survivors may share information gradually or under pressure, staff need a clear sequence of steps that guides their actions from first concern to final follow‑up.
The flow chart provides this structure by outlining who to notify, what safety checks to complete, how to document the incident, and when emergency procedures must be activated.
These types of incidence reporting flow structures are common for many organizations, but they do not always follow survivor-led or GBV principles
Each organisation should adapt the details to its own staffing and legal requirements to support a safe, coordinated, and trauma‑informed response to TFGBV.
We have provided a sample incident report flow chart, which should be updated to include roles, responsibilities, and organisation-specific practices to accompany each step.
The typical sample incident report flow chart is as follows:
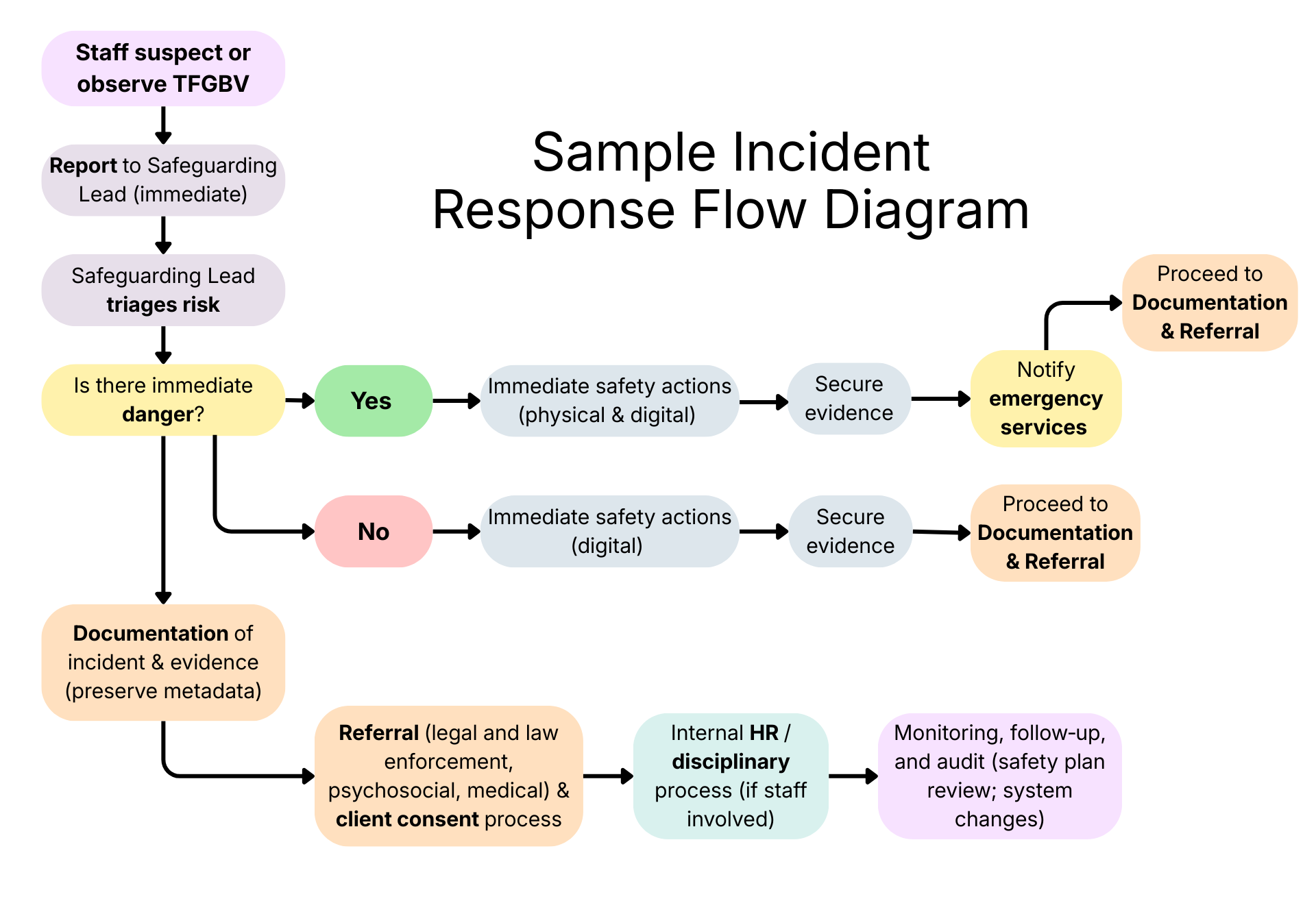
What should we do instead?
To help guide the development of your own responses, we have added survivor-centered processes to the sample flowchart. You can view these changes in the diagram below:
Practical risk assessment and intake checklists
After initial disclosure, providers must assess risk across both clinical and digital domains. This assessment guides immediate safety actions and determines which referrals are most urgent.
- Clinical risks may include threats of physical harm, suicidal ideation, lack of safe housing, or limited social support.
- Digital risks may include device or account access by the perpetrator, spyware, image‑based abuse, doxxing, location tracking, online harassment, or other forms of TFGBV.
According to your service or institutional scope, you may also want to develop a combined intake checklist that flags:
- Immediate danger (requires emergency services)
- High digital risk (requires digital‑forensics referral)
- Psychosocial needs (requires counselling or support services)
Immediate danger that require calls for emergency or immediate reporting can include the following…
- Threats of physical or sexual violence delivered through digital means, especially when they include location details, stalking patterns, or timelines.
- Real‑time stalking or tracking, such as live GPS monitoring, forced location sharing, or evidence that someone is on their way to the victim’s physical location.
- Compromised safety-critical accounts, like access to home security systems, medical devices, financial accounts, or communication channels the person relies on for safety.
- Non‑consensual intimate image release that is happening now or is being used to coerce immediate compliance.
- Escalating harassment that shows clear intent to harm or that coincides with in‑person threats or breaches of physical boundaries.
- Digital abuse that prevents someone from calling for help, accessing medication, contacting support, or finding a safe shelter.
As a service provider, you must be transparent about your role’s mandatory reporting obligations and any limits to confidentiality at the beginning of conversations.
Immediate Digital Safety Strategies
Once risks are identified, providers may support immediate digital safety steps. These actions must be taken carefully, especially when device monitoring is suspected. Immediate safety strategies (with informed consent) include:
- Change passwords from a trusted device not accessible to the perpetrator.
- Enable two‑factor authentication on critical accounts.
- Turn off location sharing and make social accounts private.
- Preserve evidence (screenshots, message headers, timestamps).
- Use a temporary “safe device” if monitoring is suspected.
- Avoid deleting messages until a forensic specialist advises.
Safety Note:
Changing any typical digital behaviour (changing passwords, logging out of or deleting accounts, turning off location, uninstalling apps) may alert an abuser. Ensure that the survivor has a safe shelter before making changes, and opt to use different devices and accounts other than the accounts which are accessible to the abuser.
Reflect
Consider the risks of altering device settings when a client’s device may be monitored, and identify strategies to reduce those risks.
Documentation Standards
Accurate, secure documentation is essential for safety planning, continuity of care, organisational accountability, and potential legal supports. Documentation should include:
- Date, time, and setting of the disclosure
- all individuals present
- Client’s statements (verbatim)
- Observed behaviour and communication needs
- Evidence collected and consent status
- Referrals made and agreed next steps
Records must be stored securely with restricted access and clear data retention and deletion policies.
Accessibility and power dynamics
When TFGBV intersects with disability, its experience and safe response may be impacted by factors such as caregiving relationships, and communication barriers. Providers must ensure that their approach does not reinforce existing power imbalances. Service providers should:
- Use the client’s preferred communication mode (sign language, text, pictorial aids, assistive tech).
- Recognise that caregivers or staff may monitor devices; plan private, safe ways to communicate.
- Adapt phrasing and pacing for cognitive or sensory needs.
Legal, ethical, and data‑protection considerations
Legal and ethical obligations shape how information is collected, stored, and shared. Providers should:
- Explain confidentiality limits and mandatory reporting obligations clearly.
- Obtain informed consent before sharing evidence; use plain‑language consent forms.
- Store sensitive records securely and follow relevant data‑protection laws and organisational policies.
Reflect
How might your documentation practices need to change to better protect TFGBV‑related data?
Ongoing safety planning
Safety planning is not a one‑time event; it is an evolving process that adapts to the survivor’s changing circumstances.
- Develop a physical safety plan. Identify important safe contacts, emergency numbers, safe locations.
- Develop a digital safety plan. Consider safe devices, password rotation, trusted backups, and a plan for social media privacy.
- Follow‑up. Schedule check‑ins, update risk assessment, and revise the plan as needed.
A well‑structured safety plan supports both immediate protection and long‑term sustainability.
Building partnerships and referral networks
No single service can address all aspects of TFGBV. Effective response depends on strong partnerships across sectors. Organisations and service staff should:
- Map local forensic, legal, psychosocial, and shelter services. You can see some examples of organisations in this textbook in on the following pages:
- Establish referral agreements and rapid‑response pathways with local resources to create an accessible network of support for survivors.
- Train staff in digital‑evidence preservation and trauma‑informed, survivor-directed care.
Partnerships can strengthen the organisation’s capacity to respond comprehensively and consistently.
Reflect
Which local partners could strengthen your organisation’s TFGBV response?
Responding to TFGBV requires a structured, trauma‑informed, and disability‑inclusive approach. By applying the AVDR framework, conducting thorough risk assessments, documenting safely, and maintaining strong referral networks, frontline providers can offer survivors meaningful protection and support.
When these practices are consistently applied, organisations strengthen their overall readiness and ensure that survivors receive responses that are safe, respectful, and empowering.
Resources
- UNFPA. (2019). The Inter-Agency Minimum Standards for Gender-Based Violence in Emergencies Programming. United Nations Population Fund. https://gbvaor.net/sites/default/files/2019-11/19-200%20Minimun%20Standards%20Report%20ENGLISH-Nov%201.FINAL_.pdf
- Women’s Shelters Canada. (2026). Toolkits. Women and Gender Equality (WAGE) Canada. Tech Safety Canada. https://techsafety.ca/resources/toolkits

Feedback/Errata