
📈 Chapter 5: Room for Improvement. Change from the Ground Up
39 5.5: Anti-Racism Education
Curriculum Integration
Educators should prioritize integrating EDI content into dietetics curricula. This involves evaluating and redeveloping intentional anti-racist student and staff recruitment practices and policies, incorporating topics such as cultural competency, social determinants of health, and anti-racism training into coursework to ensure students are equipped with the necessary knowledge and skills to address ABR in their practice. Inviting guest speakers from diverse backgrounds and incorporating diverse case studies can enhance students’ learning experiences.
Wellington et al. (2021) emphasize that integrating experiences from equity-seeking students into dietetic education is crucial for fostering an inclusive learning environment. Their research highlights that dialogue and reflection on these experiences can reveal the systemic barriers and biases faced by students from marginalized backgrounds. By incorporating these perspectives into the curriculum, educators can better address the needs of all students and promote a more equitable and supportive educational environment.
Video 5.5: Researcher and Associate Professor Eric Ng highlights the importance of starting anti-racism education and the value of learning from shared experiences.
ABR Training
ABR training involves structured educational programs designed to enhance understanding and skills related to Anti-Black Racism within dietetic practice. This includes workshops, seminars, and online courses that focus on anti-racism, cultural competence, and social justice. Training aims to improve awareness and provide practical tools for addressing racial disparities in dietetics (Public Health Agency of Canada, 2019).
Professional Development: Continuing education opportunities should be made available to RDs to enhance their understanding of ABR and its implications for dietetic practice. This may include workshops, seminars, or online courses focused on anti-racism, cultural competence, and social justice. Professional organizations can also provide resources and certifications in ABR training (Public Health Agency of Canada, 2019).
Case Studies and Role-Playing: Incorporating case studies and role-playing exercises into ABR training can provide practical examples of how to navigate complex situations related to race and ethnicity in dietetic practice. These interactive learning experiences allow RDs to develop skills in addressing ABR in real-world scenarios. Facilitators should ensure that these exercises are based on real-life situations and include diverse perspectives (Public Health Agency of Canada, 2019).
Equity Diversity and Inclusion
EDI refers to principles and practices aimed at creating fair and inclusive environments by addressing and dismantling systemic biases and promoting diverse perspectives. Integrating EDI involves adopting policies and practices that respect and value individual differences, and actively working towards eliminating barriers that marginalized groups face (Public Health Agency of Canada, 2019). Here are a few simple examples of what this looks like in practice:
- Show Respect for Individual Experiences, Perspectives, and Autonomy: At a follow-up appointment, your client discloses they were not able to follow the care plan. They explain it is too costly to purchase fresh fruits and vegetables and lean proteins. You ask the client to share their eating, cooking, and food sourcing habits. By becoming familiar with their understanding of healthy eating, you can work with them to identify the foods and services they enjoy and have easy access to, that will also meet your healthy eating recommendations.
- Educate Yourself and Spread Awareness: You notice the curriculum is centered around European eating practices. You want your nutrition care skills to be flexible in meeting the needs of diverse clients and begin researching cultural foods and practices. Once you have a foundation of knowledge, you share your concerns with one of your course instructors and ask that they incorporate diverse perspectives into the remaining course content.
- Speak Up When You See Prejudice and Unfair Treatment of Others: You are the lead practitioner in a family health team. The doctor, a woman of colour, goes into the waiting room to get her next patient. The patient says, “You can’t be my doctor, you must be the receptionist.” After the doctor politely explains their credentials, the person insists they want another doctor. You intervene and explain to the patient that their remarks are unacceptable and will not be tolerated. Your team provides a referral for the patient to see another doctor.
- Lead Change in Professional/Academic Settings to Improve Quality of Life for All: You are a dietitian in a local public health unit recognized as a food desert where many of the citizens lack access to affordable fresh produce that is appropriate for their cultural needs. You create a group led by the citizens to secure funding for subsidized food baskets that can be distributed to families that sign up on a biweekly basis. The program also features weekly storytelling sessions and cooking workshops where community members can share their meanings of food and recipes. An important feature of the program is all community facilitators are compensated for their time (Public Health Agency of Canada, 2019).
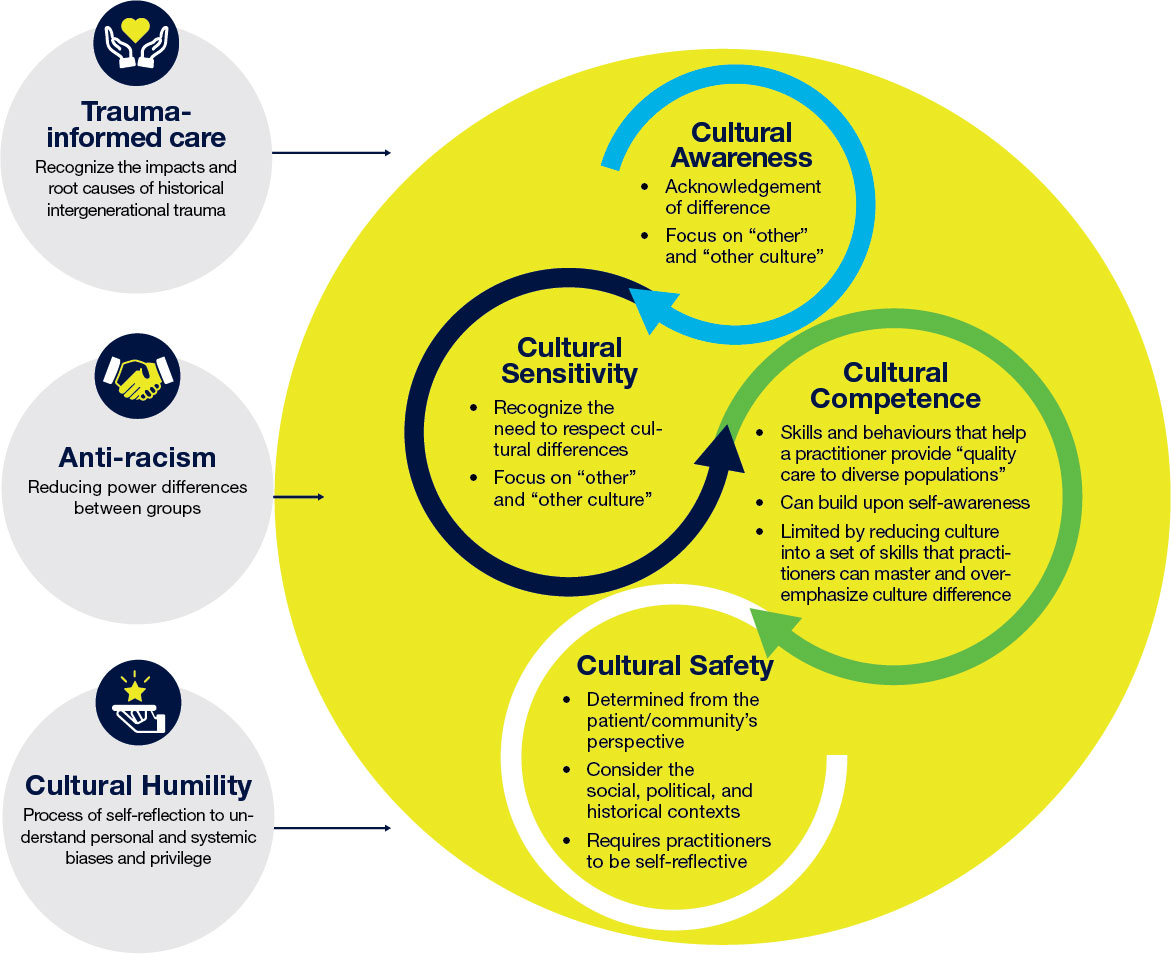
Cultural Safety
Cultural safety is a concept that ensures healthcare practices are delivered in a manner that is respectful of, and tailored to, the cultural needs of clients. It involves creating environments where individuals feel safe to express their cultural identity and are not subject to discrimination or bias (Public Health Agency of Canada, 2019).
Reflective Practice: RDs should engage in reflective practice to examine their own cultural biases and assumptions. This self-awareness is essential for providing culturally safe care to clients from diverse backgrounds. Reflective practice can be facilitated through journaling, peer discussions, and supervision sessions.
Client-Centered Care: Practicing RDs should prioritize client-centered care from a place of cultural safety, that respects and validates the cultural identities and lived experiences of individuals. This involves actively listening to clients, acknowledging their perspectives, and tailoring interventions to meet their unique needs. Client-centered care also requires understanding cultural food practices and preferences, and being flexible in dietary recommendations.
Cultural Humility
Cultural humility involves an ongoing process of self-reflection to understand personal and systemic biases, and developing and maintaining respectful relationships based on mutual trust. It requires acknowledging oneself as a learner and understanding the impact of systemic oppression, such as racism, on different populations. Incorporating cultural humility into dietetic education involves creating curricula that emphasize self-reflection, systemic analysis, and respectful engagement with diverse perspectives.
“A process of self-reflection to understand personal and systemic biases and to develop and maintain respectful processes and relationships based on mutual trust. Cultural humility involves humbly acknowledging oneself as a learner when it comes to understanding another’s experience.” (First Nations Health Authority, n.d.)
Keyword: Multicultural Education
Additional Resources
To expand your knowledge take a look at this article by the Public Health Agency of Canada:
- Public Health Agency of Canada. (2019 December). Addressing Stigma: Towards a More Inclusive Health System.