
Chapter 3 – Respiratory System Assessment
Posterior and Lateral Thorax – Palpation
The steps in palpating the posterior and lateral thorax are as follows (see Video 3.6):
1. Begin by using the dorsa of your hands to compare temperature bilaterally from the apex to the bases. Temperature should be equal bilaterally and typically warm to touch.
2. While comparing bilaterally, use the finger pads of your dominant hand, palpate the posterior and lateral thorax from the shoulders and axillary area to the bottom of the thoracic cage for pain, moisture, , masses, swelling, and .
While doing so:
- Ask the client if they have any pain. Remember to use other words that may resonate with them, such as tenderness. Pain can be associated with many different underlying pathologies, so you should further assess the pain and other related cues that provide information about the pathology and the required intervention.
- Note any moisture.
- Note the location, size, and description (hard, soft) of any deformities, masses, or swelling.
- Note the location of any crepitus. Crepitus feels like a crackling under the skin similar to popping bubble wrap. It is an acute condition related to subcutaneous emphysema in which air shifts out of the lungs and into the subcutaneous tissues as a result of traumatic, surgical, or infectious causes. It usually resolves when the acute condition is treated. However, it is important to monitor the client for any signs of respiratory distress and and if the crepitus worsens (expands in size across the chest). New onset crepitus should be examined further, and any additional respiratory changes should be assessed. The physician/nurse practitioner should be notified of the findings.
Video 3.6: Palpation of posterior and lateral thorax
3. Assess for tactile vocal fremitus, which is a vibration felt on the chest wall produced by the sounds of vocalization (speech) transmitting through lung tissue. See Video 3.7. This assessment is not commonly performed, but it can provide information about pathological conditions that cause in the lung tissue (e.g., tumour, pneumonia) or increased amounts of air (e.g., pneumothorax, emphysema). Combined with other potential cues, the findings from this assessment will point to whether further diagnostic testing is required.
- Place the ulnar or palmar surface of your fingers on about three to five locations on each side of the posterior thorax and about three locations on the right lateral thorax and two locations on the left lateral thorax (again, the number of locations depends on the size of the thorax). See Figure 3.13 for the pattern. The ulnar and palmar surface of fingers are used because they are most sensitive to vibrations.
- Begin at the apex of the lungs (near the shoulders) or just under the axilla and continue down to the base of the lungs (at the bottom of the thorax cage).
- Ask the client to say a word that produces a low-frequency sound (e.g., “foodie” or “coin”) each time you place your hands on the thorax. You may need to ask them to speak a bit louder than normal. The best words to have them say are ones that have two vowels within a single syllable because this produces a low frequency. If you are interested, a history of the words used can be found at: https://onepagericu.com/blog/tactile-fremitus-lost-in-translation
- Note the equality of fremitus in comparison from the left to the right side. The vibrations should be equal. The vibrations will be more difficult to feel as you get closer to the bases because you are further away from the larynx.
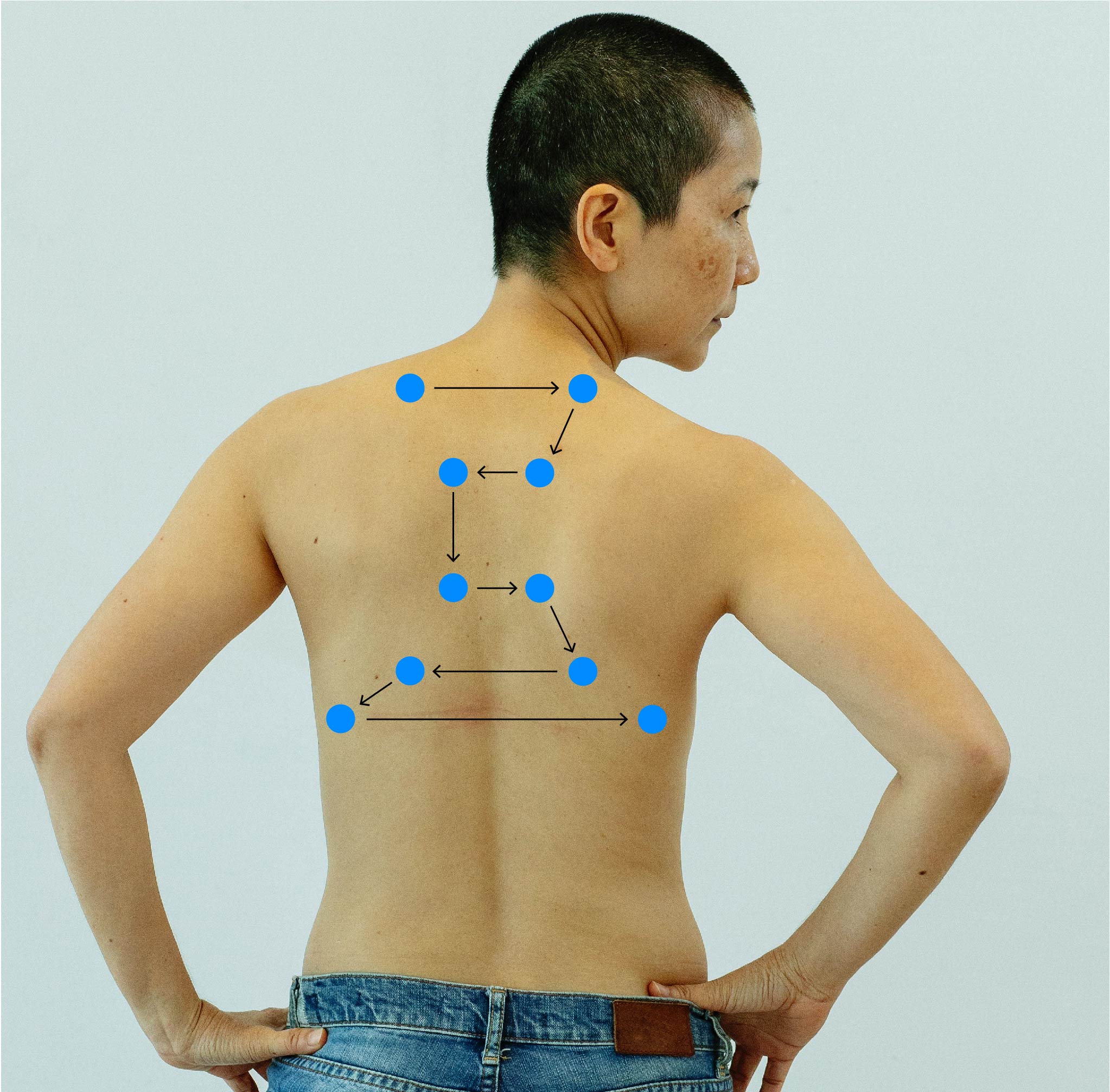
Figure 3.13: Pattern for palpation of tactile vocal fremitus
Photo by Michelle Leman from Pexels (image was cropped and illustrated upon for the purposes of this chapter)
Video 3.7: Palpation for tactile vocal fremitus
4. Note the findings
- Normal findings might be documented as: “Upon palpation of posterior chest wall, client reports no pain, temperature warm to touch, equal bilaterally, no moisture, masses, swelling, or deformities, equal tactile fremitus.
- Abnormal findings might be documented as: “Upon palpation of posterior chest wall, client reports pain inferior to scapula at scapula line, a small protrusion noted at same location, temperature warm to touch, equal bilaterally, perspiration noted, equal tactile fremitus.”
Activity: Check Your Understanding
are abnormal malformations of the body.
an acute condition related to subcutaneous emphysema in which air shifts out of the lungs and into the subcutaneous tissues.
refers to the dropping of oxygen saturation via pulse oximetry.
is when the air-filled spaces of the lungs are filled with fluid or abnormal tissue.
