Nutrition support is the provision of enteral (EN) or parenteral nutrition (PN) to treat or prevent malnutrition. Nutrition support may be used to supplement oral intake. If the individual cannot eat, it can provide all of that individual’s nutritional requirements.
A basic flow diagram for assessment of nutrition support is presented below. This flow diagram can be impacted by a variety of variables but is a good representation of how to assess for enteral or parenteral nutrition. In consideration of more complex patients, you should use this diagram as a starting point for an assessment, not a comprehensive tool for decision making.
Flow diagram of how to assess nutrition support route. A full text description of the steps are presented below .
Enteral Nutrition
Enteral Nutrition is liquid nutrition provided through the GI tract via a tube, catheter, or stoma. This is the recommended route of nutrition support for patients with functional GI tracts. If the gut works, use it!
EN is associated with reduced infectious complications, and helps to maintain:
gut integrity (supports gut barrier function)
normal digestive and absorptive capabilities
gut-associated immune function
Indications & Contraindications
Indications for enteral nutrition include a functional GI tract and clinical conditions in which oral intake is impossible, inadequate or unsafe.
Such clinical conditions include:
Neurological disease/ dysfunction (e.g. stroke, dysphagia, head trauma, head and neck cancer, decreased level of consciousness)
Enteral feeding tubes may enter the body at several different sites. The choice of enteral feeding route depends on several factors, such as the intended duration of nutrition support, the patient’s condition, and any limitations to access (such as trauma or obstructions).
Sites of Delivery
Overview of enteral sites of delivery
Sites of delivery
Access types
Indications
Advantages
Disadvantages
Gastric
(stomach)
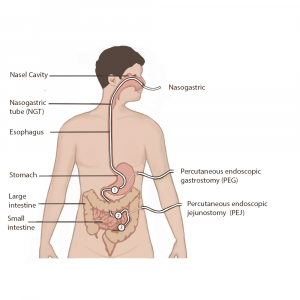
Nasogastric (NGT)
Orogastric tube (OGT)
Percutaneous Endoscopic Gastrostomy (PEG)
Gastrostomy tube (G-Tube)
Patients with normal emptying of gastric and duodenal contents
Large reservoir capacity of the stomach
Maintains normal gut function
Most cost effective
Easiest to insert
PEG/G-Tube decreases the risk of tube displacement
Can give bolus feeds
Increased risk of esophageal reflux and/or pulmonary aspiration
NGT may result in discomfort for patient and tube displacement
PEG/ G-Tube increases risk of irritation and infection at insertion site
Duodenum
(small bowel)
Nasoduodenal tube (NDT)
Oroduodenal tube (ODT)
Patients who have impaired gastric emptying or who are at risk of esophageal reflux
Normal intestinal function, need to bypass stomach
Can be used for early enteral feeding
May reduce risk of esophageal reflux or pulmonary aspiration
May require a pump to control feeding rate
May require fluoroscopic or fibre-optic endoscopic placement of tube
Risk of displacement/migration back into stomach
No gastric acid barrier against bacteria
Jejunum
(small bowel)
Nasojejunal tube (NJT)
Jejunostomy tube (J-Tube)
Percutaneous Endoscopic Gastrostomy with jejunal extension (PEJ)
Normal intestinal function, need bypass the stomach
Can bypass an upper GI surgical site, obstruction, pancreas
Can be used for early enteral feeding
May improve tolerance to enteral feeding to meet nutritional requirements and avoid parenteral nutrition
Potential gastrointestinal intolerance (bloating, cramping, diarrhea) due to lack of reservoir capacity
Requires a pump to control feeding rate
May require fluoroscopic or fibre-optic endoscopic placement of tube
Risk of displacement/migration back into stomach
No gastric acid barrier against bacteria
Delivery Methods
Overview of delivery methods, by feeding type
Type of Feeding
Explanation
Advantages
Disadvantages
Continuous Feeding
Defined as feeding over 20-24 hours either by gravity drip or a feeding pump
Continuous feeding at a low volume is often used when starting an enteral feeding regime
It is the preferred method of delivery for GI intolerance, critical illness and some medical conditions
Allows the lowest possible hourly feeding rate to meet nutrient requirements
Better gastrointestinal tolerance due to the low feeding rate
Physical attachment to the feeding apparatus (may affect quality of life)
Expense of equipment (pump and giving sets)
Cyclic/ Intermittent Feeding
Defined as feeding over 8-20 hours
Cyclic feeding involves continuous feeding over a shorter time period
Intermittent feeding involves breaks in continuous feeding administration i.e. being fed over 4 hours 3 times a day for a total of 12 hours.
Suitable for pump and gravity drip
Allows freedom from feeding equipment (may improve quality of life)
Provides breaks for physical activity, movement, medication administration with drug-nutrient interactions, lying flat to sleep, and hunger/satiety to encourage oral intake if applicable.
Useful in the transition from continuous to bolus feeding, or from tube feeding to oral intake
A higher infusion rate is required to provide the same volume of nutrition
Nutritional regimes may have a period of decreased tolerance as the patient adjusts to the new feeding rate
Bolus Feeding
A prescribed volume of feed, administered in a shorter feeding time (such as 100-400ml over 15-60 minutes), which may be repeated in intervals to achieve the required volume
Usually fed into the stomach
Physiologically resembles a more typical eating pattern promoting hunger/ satiety
Allows greatest freedom from feeding equipment
Can be used to supplement oral intake
Can be more flexible to suit the patient’s lifestyle and improve quality of life
Large boluses may be poorly tolerated, especially in small bowel feeding
Some risk of aspiration, reflux, abdominal distension, diarrhea and nausea
Enteral Nutrition Assessment
When starting an enteral nutrition assessment, it is important to use a systematic process:
Complete a thorough nutrition assessment: past medical history, history of presenting illness, laboratory values, medications, nutrition history, anthropometrics, physical assessment, risk of refeeding syndrome, medical plan, and disposition.
Determine feeding access: gastric vs. small bowel (duodenal vs. jejunal); short term or long term.
Determine protein, energy, fluid requirements.
Check for other sources of nutrients: IV infusions or solutions, medications.
Depending on your patient, you may need to consider other factors in your assessment. However, this is a general representation of the assessment process.
Background complete! Feel free to review any resources and move to the next section, “Assess”, when you are ready.