
Outpatient GI
Plan
Page Contents

Common PES Statement Terminology
As you interpret the dietary data from the assessment, you can form Problem, Etiology, Symptoms (PES) statements or nutrition diagnoses that help identify nutrition concerns that need to be addressed in your plan. If you are not familiar with how to write a PES statement please review this resource from the Academy of Nutrition and Dietetics.
Here are some common nutrition problems that clients may experience:
- Excessive energy intake
- Not ready for diet/lifestyle change
- Inappropriate intake of types of carbohydrate
- Inappropriate intake of types of fats
- Limited food acceptance
- Inadequate vitamin/mineral intake
- Inadequate fiber intake
- Food- and nutrition-related knowledge deficit
- Physical inactivity
- Unintended weight loss
- Altered nutrition-related laboratory values (specify)
- Disordered eating pattern
- Inability to manage self-care
- Impaired ability to prepare foods/meals
- Limited adherence to recommendations
PES Statements for Christian
Here is a brief list of potential PES statements for Christian. At this stage, the problem is mostly related to a lack of nutrition education in the past and a willingness to make changes.
- Food and nutrition related knowledge deficit related to a lack of previous disease specific education from a dietitian as evidenced by client report and dietary/lifestyle history.
- Not ready for diet changes related to a lack of desire to remove “trigger” foods as evidenced by clients resistance to remove coffee and alcohol from diet to relieve IBS and GERD symptoms.
- Inappropriate food intake related to knowledge deficit as evidenced by the consistent consumption of traditional “trigger” foods for GERD and IBS (tomatoes, onions, garlic, spices, caffeine, alcohol).
- Inadequate physical activity as evidenced by client report (under 150 minutes per week guideline).
Management of
Counsel the client on dietary and lifestyle triggers for GERD, and build a strategy to manage them closely for 2-4 weeks. Reintroduce foods as tolerated and depending on symptoms. Please note that triggers may vary, and restrictive diets may not be appropriate for all individuals.
Christian’s Medication and Laboratory Values
As previously mentioned in the Assess stage, Christian was experiencing heartburn, regurgitation, and hiccups before starting his medication. Christian hopes to reduce or remove the medication entirely, so it is important to provide him with education and strategies for the relief of symptoms.
When considering Christian’s management for GERD, it is also important to consider the potential adverse effects of his medications.
We know the following about Christian:
- He has been taking Nexium (a proton pump inhibitor) for his GERD for 4 weeks
- He has low serum iron and ferritin and is on the low-normal range for vitamin B12.
- He reports that he experiences extreme fatigue, headaches, and lightheadedness. Although these symptoms may be attributed in part to other lifestyle factors, you should consider his laboratory values in the context of these symptoms (as they are common).
As vitamin B12 and iron are nutrients of concern when taking proton pump inhibitors (PPI’s) for extended periods of time, it is important to consider that Christian already has low laboratory values.
Consider the recommendation of an iron and vitamin B12 supplement, if it is appropriate and aligns with your clients needs. You may or may not consult with the interdisciplinary team regarding supplementation (it is not necessary, but you may want to in some cases depending on the client and care plan).
Dietary Strategies
These are dietary strategies to help individuals manage their GERD symptoms:
- Avoid foods that increase gastric pressure: e.g. anything carbonated.
- Avoid foods that relax the Lower Esophageal Sphincter (LES): e.g. hot sauce, mints (spearmint, peppermint), fried foods, fatty foods, spicy foods, chocolate, caffeine, and alcohol.
- Eat smaller meals throughout the day: 5 – 6 meals is ideal. Large meals take a longer time to empty from the stomach, exerting pressure on the LES.
- Slow your eating and drinking: Eat and drink slowly, and chew foods well. Do not use straws or chew gum.
- Avoid foods and beverages below pH 4: In some cases, symptoms can be managed through avoiding foods and beverages like pineapple, strawberries, coca cola, cognac, cranberry juice, and yellow mustard. You may obtain detailed lists for this.
- Avoid other common triggers: e.g. citrus fruits and juices, tomatoes, chocolate, onions, garlic, and spicy foods.
Christian’s Dietary Data: GERD Trigger Foods
In consideration of dietary recommendations for the management of GERD, it is important to highlight key foods that may be contributing to Christian’s symptoms. In Christian’s case, this is his first appointment with you. It is important not to overwhelm him with suggestions. Instead, focus on key ”trigger foods” and “simple recommendations” such as swapping apples, tomatoes, onions, garlic (spices or seasoning) for other types of vegetables, and reducing caffeine and alcohol intake. Reducing consumption of these foods aligns with dietary management strategies for GERD.
| Meal | Christian’s diet recall |
|---|---|
| Breakfast 6 am | Fruit smoothie (strawberries, apple*, avocado, kale, cucumber, almond milk), 2 hard boiled egg or ”egg muffins” with spinach mixed in, and 1 large coffee with 2 cream (5%)* |
| Lunch 12 pm |
Premade salad or rice bowl (spring mix or brown rice, marinated or spiced baked chicken, cucumber, tomato, green pepper, onion, chick peas or kidney beans, walnuts, and feta or goat cheese with an olive oil dressing or any “light” dressing available), 1 large coffee with 2 cream (5%)* |
| Dinner 5 pm |
6 oz baked fish, chicken, or beef, with mixed roasted vegetables (broccoli, cauliflower, asparagus, potatoes cooked in olive oil with garlic, paprika, and other spices*), and 1 cup of quinoa, rice, or whole grain pasta |
| HS snack 11 pm |
1-2 glasses of red wine*, 1-2 cookies or 2 cups of popcorn or carrots with red pepper hummus |
Lifestyle Strategies
While it may not be a concern during an initial appointment, physical activity is an important lifestyle strategy and can be addressed at a follow-up.
Clients can be encouraged to complete:
- 150 minutes of moderate to vigorous aerobic exercise every week (e.g. 30 minutes, five days a week)
- Resistance exercises (like lifting weights) two to three times a week
It some cases, it may be beneficial to refer clients to the physiotherapist to be:
- Assessed for conditions that might place them at increased risk for an adverse event or injury during certain exercises
- Supervised by an exercise specialist for a certain period of time to ensure safety
In addition to being physically active, here are more lifestyle strategies to help individuals manage their GERD symptoms:
- Practice stress management
- Avoid alcohol or smoking
- Do not lie down for 2-3 hours after eating
- Try raising the head of your bed to avoid laying flat at night
- Avoid wearing tight clothing around your stomach and chest
- Maintain a healthy weight: Consider this strategy in the context of your client’s history and goals. Many normal and underweight individuals experience GERD and it may not be the most crucial factor for your client. Always consider that weight is not a modifiable factor for everyone and may not be realistic for your client.
Christian’s Lifestyle Habits
In addition to reviewing dietary data, lifestyle habits play an important role in managing GERD and IBS. After you discuss with Christian, he provides you with the information regarding his willingness to make changes to his lifestyle habits that may help relieve GERD symptoms.
- Christian reports eating quickly during meals, especially during breakfast and lunch as his workdays are busy. After discussion, Christian will try to eat his meals slowly.
- Christian does not have time to take a “snack break” during the workday. After discussion, Christian prefers to eat three meals a day and does not want to worry about snacks.
- Christian reports sleeping from 12:00am – 6:00am. After discussion, he recognizes that he should be sleeping more, which may help reduce his stress levels. He is willing to go to bed at 11:00pm.
- Christian reports wearing tight clothing (his business attire is a suit). After discussion, this is not negotiable.
- Christian exercises 2 times per week for 60 minutes, which does meet the guidelines (~150 minutes per week). He is not currently interested in engaging in more physical activity. Since dietary concerns are of greater importance at this stage of his nutrition care, there is no physical activity plan at this time.
Management of IBS
Elimination diets are often used for IBS. The elimination diet (which will be explained later on) has a growing body of evidence but is still widely criticized. There are “traditional food triggers” that can be explored before using a restrictive or elimination diet, such as FODMAP. Using a FODMAP diet requires commitment and dedication for it to be effective, which may not be necessary.
It is up to the dietitian and client to determine the need for an intensive strategy, but it may be best to explore “traditional triggers first” using a food symptom journal.
Food Symptom Journals
Keeping a food and symptom journal is critical to improving digestive symptoms. By consistently tracking multiple factors that relate to your digestive system, you can identify what may be triggering symptoms and truly relieve digestive symptoms.
During an initial appointment for IBS, it is important to provide a detailed explanation of the food symptom journal and the expectations for documenting. This will help the client understand and provide you with the best information for assessment, recommendations, and plans. Keeping a food symptom journal for 1-2 weeks before a follow-up appointment is often the first “plan of action.”
A food symptom journal can be kept in a table format, and should include the following headings:
- Day and time: what time of day you eat
- Food and beverages: exactly what you eat and drink (including condiments, sauces, and seasonings)
- Environment: where you are eating (homemade or outside food) and what’s going on that day (e.g. stress levels, people around you, events, eating behaviors, etc.)
- Symptoms and severity: indicate symptom severity on a scale of 1 to 5. Often the client will choose 2-3 symptoms that are affected by the most and focus on those when recording; they can denote symptoms with a letter for ease of recording
- Bowel movements: indicate number and consistency according to the Bristol Stool Scale
Bristol Stool Scale
The Bristol stool scale is a diagnostic tool that you can provide clients for explaining the appearance of their stool. The scale classifies stool into seven types, listed and depicted in the table and image below.
| Type | Description | Indication |
|---|---|---|
| Type 1 | Separate hard lumps | Constipation (severe) |
| Type 2 | Lumpy and sausage like | Constipation (mild) |
| Type 3 | A sausage shape with cracks in the surface | Normal |
| Type 4 | Like a smooth, soft sausage or snake | Normal |
| Type 5 | Soft blobs with clear-cut edges | Lack of fibre |
| Type 6 | Mushy consistency with ragged edges | Diarrhea (mild) |
| Type 7 | Liquid consistency with no solid pieces | Diarrhea (severe) |
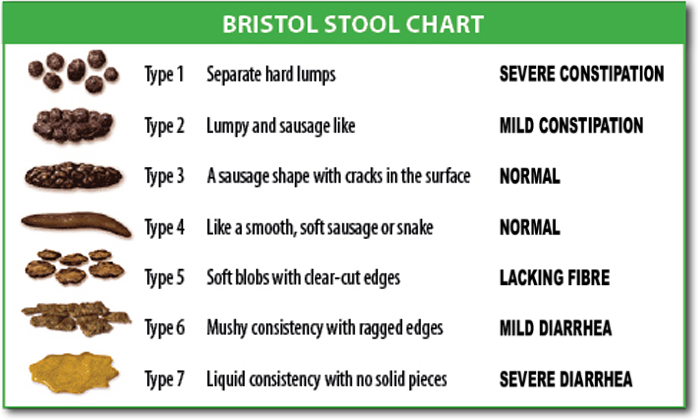
Source:Cabot Health, CC BY-SA 3.0, via Wikimedia Commons
Traditional Trigger Foods and Beverages
This list can serve as a reference point for you and the client to identify common “trigger foods” and as a first step to resolve symptoms before consideration of an elimination diet (e.g. FODMAP).
- Avoid or limit caffeine and chocolate
- Avoid all preservatives and artificial flavours
- Avoid most raw fruits and vegetables
- Avoid wheat
- No alcohol
- No cabbage in any form (e.g. cauliflower, cabbage, broccoli, brussels sprouts)
- No corn or popcorn
- No onion or garlic
- No red meat or deli meats
- No spices (e.g. cinnamon, curry, chili powder, black pepper cumin)
- No vinegars or anything fermented
- No whole seeds or nuts
Consider using a more comprehensive list during your practice.
Christian’s Dietary Data: IBS Trigger Foods
The plan for Christian’s IBS is to start with him using a food symptom journal to track his patterns over the next 1-2 weeks. He will come back with a strong representation of his habits (both dietary and environment). Managing IBS is trial and error, with a combination of various strategies, so the more we know about the person, the better.
In the meantime you can start by identifying a few foods that are of concern from his dietary recall. The foods bolded in the chart are foods you may want to identify with Christian.
| Meal | Christian’s diet recall |
|---|---|
| Breakfast 6 am | Fruit smoothie (strawberries*, apple*, avocado, kale, cucumber, almond milk), 2 hard boiled egg or ”egg muffins” with spinach mixed in, and 1 large coffee with 2 cream (5%)* |
| Lunch 12 pm |
Premade salad or rice bowl (spring mix or brown rice, marinated or spiced* baked chicken, cucumber, tomato*, green pepper, onion*, chick peas or kidney beans, walnuts*, and feta or goat cheese with an olive oil dressing or any “light” dressing available), 1 large coffee with 2 cream (5%)* |
| Dinner 5 pm |
6 oz baked fish, chicken, or beef, with mixed roasted vegetables (broccoli, cauliflower, asparagus*, potatoes cooked in olive oil with garlic, paprika, and other spices*), and 1 cup of quinoa, rice, or whole grain pasta |
| HS snack 11 pm |
1-2 glasses of red wine*, 1-2 cookies or 2 cups of popcorn* or carrots with red pepper hummus* |
In Christian’s case:
- You can create a plan together about foods he is willing to remove (even on a trial basis) to evaluate he symptoms.
- You can give him low-FODMAP alternatives (which will be listed later on) to replace these traditional trigger foods. Note that these recommendations are similar to the ones we created for GERD.
- It is reasonable to create nutrition recommendations for both GI concerns, as they compliment each other. But in other cases, too many changes or recommendations in an appointment may become overwhelming and may not be appropriate.
- You are not going to start a FODMAP diet immediately because this is the first appointment and you should gather more information and try eliminating traditional triggers first
FODMAP Diet
FODMAP is an acronym for:
- Fermentable
- Oligosaccharides (Fructans & Galacto-oligosaccharides)
- Disaccharides (Lactose)
- Monosaccharides (Fructose)
- And
- Polyols (Mannitol and Sorbitol)
These are short-chain carbohydrates that have been shown to increase water volume in the small intestine and be rapidly fermented in the large intestine. This leads to increased gas production and symptoms (i.e. pain, bloating, distension, flatulence, nausea and altered bowel motility). A low FODMAP diet restricts these short-chain carbohydrates.
A low FODMAP diet is the only focused elimination-type diet that is appropriate for IBS. Even if an individual is not pursing a FODMAP diet, it is still important to understand FODMAPs and where they are found. You should seek further readings to review and become familiar with the common high FODMAP foods in each group.
Caveats
The low FODMAP diet is considered to be a second-line dietary strategy that can pursued after:
- Assessment
- Management of dietary and lifestyle factors
- Elimination of “traditional triggers”
The long-term restriction of FODMAPs is not recommended. Briefly, recent research suggests that long term FODMAP restriction carries the risk of nutritional inadequacy, has the potential to foster disordered eating, and potentially unfavourable gut microbiota (although the impact is unknown).
Structured reintroduction of FODMAPs is recommended after six weeks to identify which FODMAPs an individual is sensitive to, assess tolerance to individual high FODMAP foods, promote food variety and support long-term self-management.
The key is to find and emphasize substitutions for foods that are eliminated (as they are triggers). This is to help clients make realistic and positive changes and reduce the fear and anxiety around consuming foods.
Phase 1: Elimination
The FODMAP diet involves a three-phase approach. The first phase is “Elimination” focused on replacing foods high in FODMAPs with those lower in FODMAPs. It is very important to work with your client to ensure they are still eating a balanced diet.
Dietary strategies may include the following:
- Avoiding foods that are substantial sources of fructans (e.g. wheat, rye, onions, garlic) and galactans (e.g. cabbage, certain vegetables, legumes such as chickpeas).
- Restricting lactose-containing foods (if lactose malabsorption intolerance is present).
- Avoiding naturally-occurring and artificial polyols (e.g. stone fruits, and mushrooms, sugar-free chewing gum).
The following list acts as an example of information you may provide a client. This is not comprehensive, and if following a FODMAP diet, you will want to provide your client with a more detailed list.
| Food Category | Avoid High FODMAP foods | Choose Low FODMAP foods |
|---|---|---|
| Vegetables |
|
|
| Fruit |
|
|
| Protein sources |
|
|
| Grain products | Wheat, rye, and barley- based products, including:
|
|
| Nuts and seeds |
|
|
Phase 2: Reintroduction
The goals of the reintroduction phase are to help:
- Increase variety and re-introduction of foods quickly
- Identify foods that do and do not trigger symptoms.
Clients can reintroduce each FODMAP category one at a time to determine which foods they can tolerate and in what amounts. This process may be done gradually, rather than following a strict challenge protocol, depending on the client’s preference.
The goal is to introduce a high FODMAP food from just one category at a time, increasing the serving size over a 24-hour period to monitor for symptoms. If no symptoms occur after this trial, the next food can be reintroduced after 48 hours, assuming the client is feeling well.
During the “Personalization” phase, clients can begin adding foods back into their diet once they have identified which ones are tolerated without symptoms.
Phase 3: Personalization
Once the client has tested a variety of FODMAP categories and has a stronger clarity about individual trigger foods and/or portion sizes that are tolerable, the last step involves bringing FODMAP foods back into the diet to increase variety and nutritional quality.
At this stage, it is a balancing act between symptom management and enjoyment of food (sometimes symptom management instead of resolution is the result). It is also important to remember other factors that influence IBS symptoms, such as stress and environment.
The process for this personalization phase can be broken down into the following steps:
- Add one high FODMAP food per day
- Add another new FODMAP food the next day
- If these foods (and portion sizes) do not trigger symptoms, keep including them in your diet.
- If you experience symptoms, continue documenting in a food symptom journal to determine if this is a trigger food and return to regimen.
Probiotics and Other Supplements
Probiotics are edible, living microorganisms that may be helpful in the management of IBS. There are many probiotic products available in different doses and variable bacterial strains. Many practitioners and clients have reported improvement of IBS symptoms with probiotic use.
In general, taking probiotics for IBS is considered safe. If an individual finds four weeks of use of a probiotic is beneficial, they can continue to take it. This is a decision to be made between the client and the dietitian, in consideration of a variety of factors (adherence, effectiveness, cost).
Individuals with IBS who choose to try probiotics should be aware that some products contain other ingredients that may increase IBS symptoms (e.g. dietary fibre: oats; FODMAPs: inulin, lactose, fructose, sorbitol and xylitol).
There is currently inadequate evidence to recommend any specific probiotic product independent of IBS-subtype (constipation or diarrhea or mixed predominant IBS)
The minimum concentration of bacteria typically recommended in probiotic supplements is 1 billion CFU per dose or higher. However, some research may demonstrate the effectiveness of a smaller dose for specific strains. Most probiotics range from 1 billion – 10 billion (with some up to 50 billion).
In addition to probiotics, here is a list of other IBS management supplements that clients may ask you about:
- Digestive Enzymes
- Prebiotics
- Apple Cider Vinegar
- IBGard (peppermint)
- Biocidin (herbal)
- Candibactin (herbal)
- Ginger
It is worthwhile to explore the evidence surrounding these supplements as you may receive questions about them in practice.
Management of Celiac Disease
Although celiac disease cannot be “cured”, it can be managed effectively by keeping a strict gluten-free diet.
To help manage a client’s celiac disease:
- Look out for nutrient deficiencies: iron (in 50% of diagnosed), vitamin D, folate, B12, B6, and zinc.
- Evaluate a client’s diet for nutrients of concern (as a result of a gluten-free diet and their dietary behaviours)
- Develop strategies to provide a balanced and nutrient dense diet.
It is important to overview the following with someone who is newly diagnosed with celiac disease:
- Cross-Contamination: Individuals with celiac disease should have their own cooking supplies, utensils and condiments.
- A general list of foods to avoid and foods to include: This is a starting point to get individuals familiar with gluten-containing foods in various categories. May consider using a phone “app” for scanning barcodes or eating at restaurants as lists can be overwhelming.
- Reading food labels: even though many food companies are highlighting “gluten-free” on labels, it is important that individuals know common and “hidden” ingredients to look for.
Review the list of gluten containing foods below
Management of Diverticulitis
Preventing Diverticular Disease
Practice-based Evidence in Nutrition (PEN) suggests that the overall recommendations for the prevention of diverticular disease and acute diverticulitis are based on small amounts of low-quality evidence. However, they provide the recommendations with caution as a result of limitations in evidence.
Healthy lifestyle practices should be encouraged to prevent diverticular disease and acute diverticulitis. General recommendations include:
- Consuming a high fibre diet through dietary sources with or without supplementation (e.g. up to 20 grams per day of supplementary fibre)
- A diet high in fruit, vegetables and whole grains
- Staying hydrated
- Being physically active
- Limiting intake of red meat
- Ensuring adequate vitamin D levels
- Limiting intake of alcohol consumption and not smoking (although no significant associations have been found)
- Avoiding nuts, corn, popcorn and fruit with small seeds (e.g. strawberries, blueberries) in some cases.
- This applies mostly to those who experience an occurrence of acute diverticulitis, if they have worsening symptoms that may be related to the consumption of these foods (common triggers)
- Assess this recommendation on a case-by-case basis
A recommendation regarding probiotics cannot be made at this time. However, there is emerging data to suggest the beneficial use of probiotics for diverticulitis. Given there are no contradictions for probiotics, you and your client would decide whether probiotics may be a part of their nutrition care plan.
Managing Acute Diverticulitis
The dietary management of acute diverticulitis is different than preventing it. It is important that clients understand the difference.
If a client/patient is having a diverticular flare, they can:
- Stick to a fluid-only diet for a few days until symptoms (i.e. pain) improve.
- Eat a low insoluble fibre diet while recovering. Once symptoms resolve, patients can return to a high-fibre diet.
- Receive antibiotics, as acute diverticulitis management is often accompanied by antibiotics
Simulation Activity: Christian
To practice what you’ve learned about GERD and IBS management, complete the simulation activity below. After you complete the simulation, review a summary of Christian’s nutrition care plan.
Nutrition Care Plan Summary
Christian’s Nutrition Care Plan
Based on the details gathered prior to and during your initial appointment with Christian, here is a suggested nutrition care plan.
| Area of Concern | Recommendations |
|---|---|
| Medication and supplements |
|
| GERD & IBS Management |
|
| Dietary choices |
|
| Lifestyle habits |
|
Gastroesophageal Reflux Disease
Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols (short-chain carbohydrates)

{kind=link}